
Have you been struggling to feed through the mouth because of your condition and your doctors have suggested you have a feeding tube inserted in your stomach to help with nutrition.
Am summarising here 7 questions that I usually hear patients who come to intervention radiology ask about the RIG insertion.
For this article I will rely:
⚫ On experience and knowledge as an interventional radiographer who works with doctors performing these procedures.
⚫ And on scientific medical studies on this subject matter.
Happy reading!😀
▶️Why will your doctor request a feeding tube insertion?
There are many reasons why you may need a feeding tube. Here are some of the common reasons.
🟠You are losing weight.
🟠 You cannot eat or drink enough.
🟠Eating and drinking leads to choking or discomfort.
🟠Your breathing function is reduced, or you get chest infections.
🟠It takes a long time to eat, and it is no longer enjoyable for you.
🟠You have been getting nutrition through a tube in your nose for many weeks (nasogastric tube (NG)).
🟠The feeding tube in your nose keeps coming out.
🟠It is unsafe for you to eat or drink.
🟠Sometimes feeding tubes are placed if problems with swallowing are likely to occur.
▶️What are the potential benefits of having a RIG feeding tube inserted?
🟠To help you receive enough nourishment and fluids daily on a medium to long term basis.
🟠For some it is the safest way and the most comfortable method of feeding if you can not eat with your mouth.
🟠It also enables some medications to be given routinely through the RIG feeding tube.
▶️ What are the three types normally used for feeding tube insertion?
There are three different procedures that I have seen being used for a feeding tube insertion.
1️⃣ Percutaneous Endoscopic Gastrostomy (PEG)
2️⃣Per-oral Image Guided Gastrostomy (PIG)
3️⃣Radiologically Inserted Gastrostomy (RIG)
Of all the three types, the most common tube used is a PEG. You may only have a RIG OR PIGG inserted if you cannot have sedation or if the camera cannot access your stomach. Or any other medical reasons.
Radiologically inserted gastrostomy (RIG) is an alternative to percutaneous endoscopic gastrostomy (PEG) and for patients with eating difficulties who need long-term enteral nutrition (Smits 2020)
▶️What is the difference between these three feeding tubes (RIG) ,a PEG and a PIG tube?
A gastrostomy RIG feeding tube, Endoscopically PEG and PIGG feeding tube are used for the same purpose, only that they are inserted via different methods.
What is a Gastrostomy (RIG)
A RIG stands for Radiologically Inserted Gastrostomy – inserted using X-ray guidance after having barium placed inside the stomach.
This is a technique where a narrow plastic tube is placed through the skin into your stomach. Once in place, the tube can be used to give you liquid food directly into your stomach to provide nutrition.
What is an Endoscopically (PEG)
A PEG in full is a percutaneous endoscopic gastrostomy procedure where a feeding tube is inserted via a telescope down the food pipe.
While a per-oral image guided gastrostomy (PIG), which is less common. The tube is placed using x-ray.
The difference between them is the way they are inserted and the stage of the condition where it is appropriate for the operation to be performed, but the result is the same
So, whichever procedure your doctor has decided to use, it will be based on your needs as an individual and you will have a discussion with your doctor.
This article focuses on Radiologically Inserted Gastrostomy (RIG) to answer frequently asked questions.
▶️Is gastrostomy (RIG) a major surgery? How is it done and what are the side effects?
Having a RIG feeding tube as a planned procedure, should not worry you.
For reassurance before the procedure, you will be given plenty of time to discuss with your consultant, nutritionist and radiologist who will be performing the procedure.
I have witnessed many RIGS insertions over the years as an interventional radiographer.
And I want to reassure you that it’s a common safe nonvascular x-ray brief procedure, it is not a major surgery.
▶️Here are the steps followed during the insertion after you have been prepared.
Steps taken:
🟠The interventional radiologist will use an ultrasound probe and X-rays once your stomach is filled with air to decide the best site for the RIG.
🟠Local anaesthetic will be injected into the skin to numb the area, and you will probably be given sedation.
🟠A small needle is placed into the stomach through which a special feeding tube is placed.
🟠The doctor will attach two or three small buttons to your stomach. These are like sutures (stitches) and will secure your stomach to the abdominal wall to try and reduce the risk of infection.
🟠A wire will be passed in between these buttons. An area will be formed, and we will fit the tube.
🟠The tube will usually be held in place by a balloon at the end of the tube filled with water to help prevent the tube from falling out.
🟠The buttons attached to your stomach will stay in place for up to six weeks.
🟠They will usually fall off on their own, but a nurse may come and remove them before then.
Smits ,2020
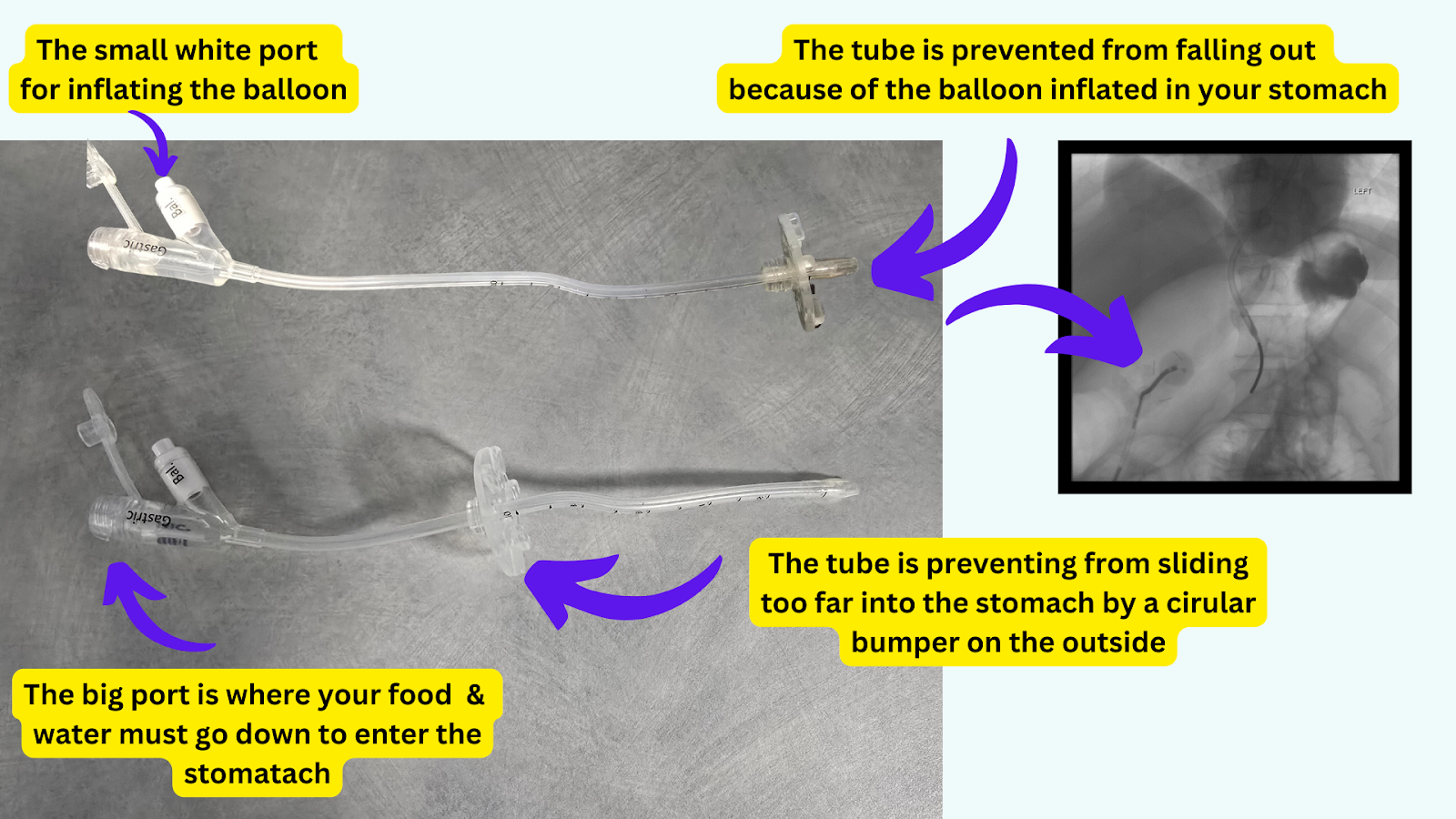
A labelled RIG tube normally used, they come in different sizes.
Usually, the feeding tube must stay in until you can eat and drink safely and normally.
Your trained dietitian, doctor or nurse will advise you on when to remove it and how to clean the tube to avoid any infection.
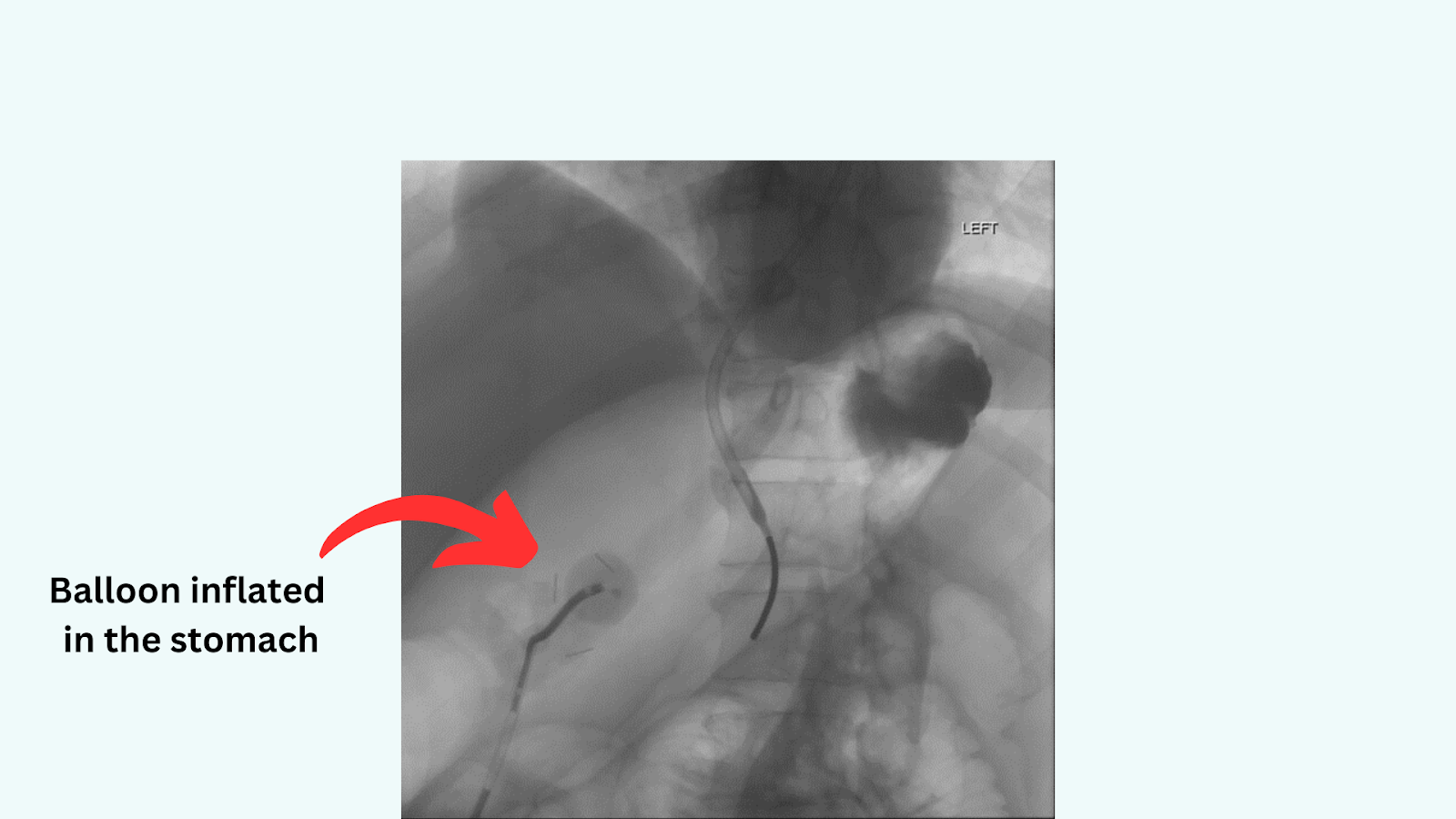
x-ray image of RIG tube inserted in the stomach showing an inflated balloon.
▶️What do studies say about the alternative of RIG, PEG and PPIG feeding tubes?
A study to compare the options of the three types of feeding tubes procedure was done and a technical success was 98 % of PEG, 100% RIG and PIG
Results:
♦️ 98% respectively inserted tubes for Antibiotic prophylaxis significantly reduced stoma infection for orally placed tubes
♦️Ten out of 50 (20%) small-bore RIG tubes blocked.
♦️Replacement tubes were required in six out of 50 PEGs (12%), 10 out of 50 RIGs (20%), but no PIGs
♦️No procedure-related complications occurred.
Laasch, 2003
So, to reassure you having one of these procedures will be for your own good. They are safe procedures that are done with care.
▶️Possible complications after the RIG insertion.
With every operation, you cannot rule out possible risks and complications. With RIG insertions complications are more common after the insertion than during the insertion.
The truth is complications remain rare (0.1 % of cases) when they do occur, they can include:
♦️ Pain at the incision site
♦️ Mild pain as a feed or medicine is given through the gastrostomy can sometimes happen.
♦️ Bleeding from the gastrostomy opening sometimes and if it happens it should be assessed as soon as possible.
♦️ Feed or stomach contents can leak from the gastrostomy opening to the lungs causing pneumonia.
♦️Infection near the incision.
♦️ Breathing difficulties can happen but are rare.
▶️Can the RIG tube fall out (dislodge) after it has been inserted?
Yes, it is possible for the tube to accidentally fall out, it’s not usually straight.
Here are some reasons why a tube can dislodge.
♦️Coughing or various activities, I have seen patients come back with a tube out.
♦️Sometimes the balloon can burst, and it loosens. It is very important that it is replaced within an hour or the hole in your stomach may close
Caution! Always consult your doctor when you experience any of these side effects or when you are concerned about something.
▶️Can you still eat with a gastrostomy tube, and do you get full when fed through the tube?
If a speech and language therapist or doctor advises you that it is safe for you to eat and drink, the tube will not prevent you from doing so
Most of the time if you do not have dysphagia, or difficulty swallowing you can still eat by mouth but always ask your doctor before you do so.
I have had patients ask this question and this will depend on a few things.
Most patients get full while feeding through the tube. And some patients can still feed through the mouth but that will depend on individual needs and condition.
Remember the main reason you are having the Gastrostomy RIG inserted is because you are having difficulty using your mouth to eat or swallow.
So, it will be wise to use the inserted feeding tube for your nutrition needs. And your doctor will be able to advise you on when you can start eating through the mouth.
You should feel less tired, hungry and thirsty than before the RIG was inserted.
Initially the dietician will work out an individual regime for you to ensure you have the correct caloric intake and nutritional balance.
Some patients I have seen feeding by mouth while they have a feeding tube are:
♦️These with no dysphagia, or difficulty swallowing problems.
♦️Only when you have been assessed by your dietitian that 60% to 75% of your calories and protein are fed by mouth, your doctor may be informed that it’s safe to remove the feeding tube.
▶️How long does a gastrostomy (RIG) insertion take to recover?
Always remember healing is different for everyone
Here are some of the proposed recovery times I have witnessed with patients we see every day in intervention.
| Stages | Timeline |
| Soreness around the site | A few days or more |
| Resting how long | Avoiding activity for the next 24 to 48 hours or more depends on the individual. |
| Feeling mild pain and rest | As healing occurs you will feel less pain. Should not last more than 3 days. |
| Recovery after the insertion | 3 to 4 days you should be feeling better or more depending on individuality. |
| Wound care | Keep the site dry for at least 48 hours |
| Remove dressing | A day after tube inserted because it does not require dressing routinely |
| Wound healing & no pain | 4 weeks and no pain. |
| Clean the tube and site | Daily |
| Resume normal activities | This will depend on how soon you recover. Some people within 24 hours |
| When can you drive | No driving after 24 hours after the procedure, only when you are not in pain & you can perform an emergency stop. |
| Bathing after the tube is inserted | No bath or shower for the first 2 days after your tube is placed, instead wash with a cloth.1 week after you may have a shallow bath, do not soak/immerse the tube and exit site.4 weeks you can do both. |
| Tube removed | Some patients for a short term, others require a RIG long term for example a study of 31.2% of patients had their gastrostomy removed within 3 years (Parr, 2024) |
| RIG is changed after the first exchange. | Every 3 months or less depends on the individual. |
▶️Will I need to keep the RIG feeding tube in forever?
No, usually if it becomes safe to swallow food and drink, and your nutrients are good, the Rig tube will be taken out.
Having a RIG feeding tube removed, is often an indication of recovery and for many patients this is a goal to aim for.
Most patients who have these tubes inserted have had long term health complications and conditions.
So, the aim is to focus on helping you understand the benefits when the tube will be removed.
This helps with coping with your feeding strategy and understanding your condition.
Some patients only have the feeding tube for a short well, then return to an oral diet, they are monitored at home more closely at home by a dietician.
A retrospective study about factors influencing RIG feeding tube removal done by Parr et al 2024 combining three teaching hospitals in the UK
Patients were included if they had received a new gastrostomy at the hospitals and were also known to the home care enteral feeding team between January 2016 and December 2019. All patients were over the age of 16
Results
A total of 451 patients who had a new gastrostomy insertion between January 2016 to December 2019.
Patients who had RIG feeding tubes inserted because of the following conditions: head and neck cancer, stroke, Parkinson disease, multiple sclerosis, cognitive impairment, poor swallow and weight loss.
The likelihood of tube removal was over 0 to 3 years, and this varied depending on the indication for which it was inserted.

Here is a table showing factors influencing gastrostomy tube removal over a period of 1,2 to 3 years (Parr et al 2024)
Nearly one third (31.2%) of all patients who underwent home care gastrostomy tube feeding went on to have their enteral feeding tube removed within 3 years and returned to oral feeding.
Parr et al 2024:
We have come to the end of this article, any questions let’s meet in the comments section
Wishing you a quick recovery!🙋
📚Source:
Smits MLJ, Tetteroo PM, Vonken EPA, Reinders MTM, Monkelbaan JF. Radiologische plaatsing van percutane voedingssondes [Radiologically inserted gastrostomy]. Ned Tijdschr Geneeskd. 2020 Dec 17;164:D5050. Dutch. PMID: 33651493.
Laasch HU, Wilbraham L, Bullen K, Marriott A, Lawrance JA, Johnson RJ, Lee SH, England RE, Gamble GE, Martin DF. Gastrostomy insertion: comparing the options–PEG, RIG or PIG? Clin Radiol. 2003 May;58(5):398-405. doi: 10.1016/s0009-9260(03)00058-8. PMID: 12727170.
Looking after your radiologically inserted gastrostomy tube (RIG) https://www.cuh.nhs.uk/patient-information/looking-after-your-radiologically-inserted-gastrostomy-tube-rig/
Parr H, White S, Loversidge C, Shiha MG, Raju SA, El Atrash MS, McAlindon ME, Hopper AD, Williams EA, Sanders DS. Factors influencing gastrostomy tube removal. Scand J Gastroenterol. 2024 Aug;59(8):1010-1014. doi: 10.1080/00365521.2024.2366968. Epub 2024 Jun 17. PMID: 38885119.
Alhasani F, Bazarah S, Ahmed M, Alraddadi B, Alotaibi A. Gastrostomy Tube Insertion Complications and Patient Care Outcomes in a Tertiary Care Hospital. Cureus. 2021 Oct 3;13(10):e18458. doi: 10.7759/cureus.18458. PMID: 34745782; PMCID: PMC8562559.