
Have you been diagnosed with a pelvis (Hip) fracture, and you have so many questions about treatment and recovery. Are you worried, wondering when you will be able to walk again?
Based on my experience as a diagnostic radiographer and on the scientific studies on the subject, I have written this article for you.
Happy reading!😀
Last updated: April 2024. Written by Juliet Semakula, diagnostic radiographer.
Disclaimer: no affiliate links.
Anatomy
Usually when you have had a Hip fracture it will be around the proximal femur.
Most hip fractures I have x-rayed occur in one of two locations on the long bone that extends from the pelvis to the knee (femur).
1️⃣ The femoral neck. This area is situated in the upper portion of your femur, just below the ball part (femoral head) of the ball-and-socket joint.
2️⃣The intertrochanteric region. This region is a little farther down from the hip joint, in the portion of the upper femur that juts outward.
Most hip fractures I see are commonly seen in the elderly following a fall. Hip fractures that occur in younger adults are often the result of high-energy trauma.
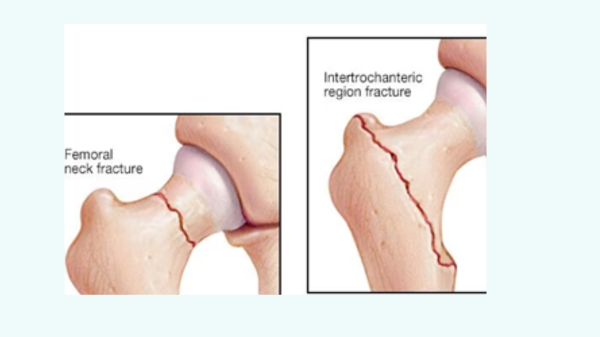
The image below shows the area where hip fractures commonly occur.
▶️ How serious is a hip fracture?
The hip fracture has a high rate of injury and death if not taken seriously.
The reason being the blood supply to the femoral head plays an important role when deciding the management of hip fractures.
The main arterial supply to the femoral head is from the medial and lateral circumflex femoral arteries. These vessels give branches that pass proximally through the joint capsule to supply the femoral head. In intracapsular fractures, these vessels can be damaged, which results in avascular necrosis of the femoral head.
By avascular necrosis I mean the death of bone tissue due to a lack of blood supply. When you break your hip the blood flow to a section of the bone can be diverted. That can lead to non-union hindering your mobility.
So, this makes hip fractures serious, Immediate treatment is needed to allow stabilisation and quick mobility.
▶️Diagnosis of hip fractures
Most hip fractures can be diagnosed on x-ray imaging alone.so your doctor will send you to have x-ray imaging to confirm if you have fractured your hip.

Image showing an intertrochanteric fracture
Only when the fracture is not visible on x-ray you will have an MRI scan taken, which is sort to be the gold standard for fractures that are not visible on x-ray and account for between 2% to 10% of hip fractures (Deleanu, 2015)
MRI has demonstrated 100% sensitivity and 93% to 100% specificity at diagnosing invisible hip fractures.
If MRI is not available, then CT is a valid alternative; however, it can miss fractures, particularly those that occur in the axial plane.(Foex, 2018)
▶️Hip fracture treatment and management.
When you go to the emergency department initial management will begin straight away to prevent any more blood loss, so you will be given fluids replacement and blood transfusion if need be.
The definitive management will depend on a few things.
1️⃣The type and location of the fracture you have got.
2️⃣Your general health and your personal preference.
The primary aim will be to help you restore mobilisation as swiftly as possible, and therefore operative intervention is normally preferred for most hip fractures.
Early surgery in hip fracture patients is linked with improved outcomes, and therefore operating within 48 hours of admission is recommended (khan,2009)
In case where you are not fit for surgery conservative management for your fractured hip will be applied. Un-displaced intracapsular fractures can be managed conservatively or surgically.
Without surgical: conservative treatment
In such cases, your doctor will give instructions to promote healing.
⏺️You will be advised to bed rest with the application of traction.
⏺️Minimal to no weight-bearing for several weeks.
⏺️You will be advised to wear a Zimmer splint to limit hip movement.
Conservative management is associated with poor function and fracture displacement (Cserhati, 1996)
But this does not mean that you will not recover from your hip fracture. Just be gentle with yourself and be patient.
Surgical management
When the doctor decides that you need surgery for your hip fracture.
Usually, they will use an open reduction and internal fixation (ORIF OR DHS or an intramedullary femur nail) procedure where a plate and screws will be used to stabilise your fracture.

Image on the left showing a intertrochanteric fracture and the right a post surgical procedure
▶️Complications following a hip fracture surgical management.
The complications following a hip fracture are vast, diverse, and multifactorial.
⭕Infection is one of the complications that can arise after your operation.
Scientific studies state the infection rates following surgical management of fractured hips to be between 0.6-3.6%, but these vary depending on the operation type.(Mackay,2000)
⭕You will also feel post operative pain. Most patients I see who come back for post x-rays are usually in slight pain, but it is always managed by painkillers.
⭕Sometimes you might have slight bleeding, neurovascular injury, and wound problems.
⭕Sometimes failure of metal work fixation, non-union and avascular necrosis.
You will be advised to take it easy in the first few days after your operation, good care and observation will be needed.
▶️The post-operative rehabilitation is as important as the initial surgery.
Can you still walk with a fractured hip?
I usually have patients ask this question, the truth is the aim of surgery is to restore mobility, and therefore early mobilisation is recommended immediately after surgery.
▶️The rehabilitation phase is divided into two:
1️⃣The first few weeks after surgery, up to the follow-up x-ray. The goal is to encourage healing by staying active without increasing pain to the joint.
2️⃣The months following the follow-up x-ray you gradually resume all your pre- activities.
Patients who have undergone arthroplasty or fixation of hip fracture can usually mobilise immediately after surgery without weight restrictions.
Regular physiotherapy will be required to encourage the rapid progression of your original mobility status.
Medical management will also be optimised to reduce the risk of associated complications.
Unfortunately, most elderly patients do not regain their previous level of mobility or independence and therefore require social care input.
So, the main objective of a physical therapy sessions is:
🔽To gradually help you gain the ability to perform all your daily activities such as walking without crutches.
🔽Implement actions to prevent the risk of falling again looking at your living environment.
🔽Monitor the gradual reduction of pain, swelling and hematoma.
▶️ How long does it take to recover from a hip fracture?
Recovering from a hip fracture will depend on an individual, some people recover much faster than others.so these average data dates in the table below, you may fall into one of the extremes or even outside of it! But be patient and you will eventually recover from your fracture.
| Hip Recovery timeline | This will depend on individual basis |
| Recovery Milestones | Timeframes |
| Disappearance of hip and thigh pain | Decrease from the first day’s post-surgery/post-fracture |
| Complete or partial disappearance 1 to 12 months after surgery | |
| Resumption of walking with canes, walker for a few metres | The day after surgery or within a few days at most |
| Resumption of walking with a walker for more than 300 metres | 1 to 3 weeks after surgery if there were no walking difficulties before surgery |
| Resumption of walking without any assistive devices | 1 to 4 months |
| Resumption of all daily activities without assistance for example cooking. | 2 to 5 months |
| Resumption of driving | 1 to 3 months |
| Return to sports | 3 to 12 months, depending on the sport and prior activity level |
Recovery timeline after hip fracture, based on NHS physical therapy professionals at north.
▶️Rehabilitation for hip fracture in elderly
An inter-professional approach should be taken to manage complex fractures of the elderly.
In this group physiotherapists play a crucial role in the post-operative care with hip fractures.
Dietician input is required to optimise nutrition to meet metabolic demands as well as to promote wound healing.
Elderly patients often will require a lot of nursing care, both pre and postoperatively.
Input from elderly medicine physicians is also crucial both pre- and post-operatively to optimise patients for surgery, manage acute medical pathologies, assess falls risks, investigate for osteoporosis, and aid with a patient’s on-going medical needs while rehabilitating.
For elderly 70 and above in most situations, it can take between nine months and one year to fully recover from this type of injury
▶️What not to do with a hip fracture after surgery?
DO NOT bend your hip more than 90o, for at least three months after your surgery.
Do not reach forward towards your feet for example to pick up something you’ve dropped.
Do not bring your knee higher than your hip when sitting for example to tie your shoes.

Try not to sit for more than 45 minutes at a time without getting up and moving around.
Choose chairs with arm rests to make it easier to stand up. Sit with your feet flat on the floor and point your feet and legs outward a little.
DO NOT cross your legs or your ankles:
⭕Crossing your legs or ankles could cause your hip to dislocate.
⭕Putting your ankle on your knee or thigh could cause your hip to dislocate.
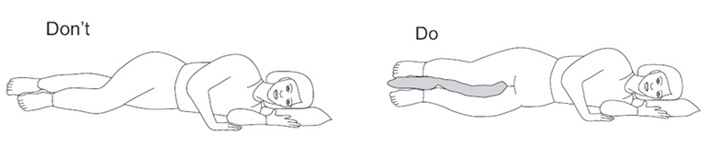
⭕Always use a pillow between your legs when you’re lying in bed.
This is what I wanted to tell you about hip fracture. I hope I have answered some of your questions, I wish you a quick recovery.🙋
Below are some of the articles I have relied on for this article.
📚Sources:
Image from https://www.mayoclinic.org/diseases-conditions/hip-fracture/diagnosis-treatment/drc-20373472
Deleanu B, Prejbeanu R, Tsiridis E, Vermesan D, Crisan D, Haragus H, Predescu V, Birsasteanu F. Occult fractures of the proximal femur: imaging diagnosis and management of 82 cases in a regional trauma center. World J Emerg Surg. 2015;10:55. [PMC free article] [PubMed] [Reference list]
Foex BA, Russell A. BET 2: CT versus MRI for occult hip fractures. Emerg Med J. 2018 Oct;35(10):645-647. [PubMed] [Reference list]
Khan SK, Kalra S, Khanna A, Thiruvengada MM, Parker MJ. Timing of surgery for hip fractures: a systematic review of 52 published studies involving 291,413 patients. Injury. 2009 Jul;40(7):692- [PubMed] [Reference list]
Cserháti P, Kazár G, Manninger J, Fekete K, Frenyó S. Non-operative or operative treatment for undisplaced femoral neck fractures: a comparative study of 122 non-operative and 125 operatively treated cases. Injury. 1996 Oct;27(8):583-8. [PubMed] [Reference list]
Mackay DC, Harrison WJ, Bates JH, Dickenson D. Audit of deep wound infection following hip fracture surgery. J R Coll Surg Edinb. 2000 Feb;45(1):56-9. [PubMed] [Reference list]