
Diabetic foot amputation is very common especially if you have diabetes mellitus, a disorder.
Are you wondering how the disease can affect the foot if not managed well and how you can prevent foot amputation? You are in the right place.
In this article I will be looking at the causes of diabetic foot amputation, proper management of our foot to avoid any future complications and I will answer the most frequently asked questions about foot amputation.
As a diagnostic radiographer I see so many patients who come for x-ray with foot amputations.
And as always I have delved into scientific medical studies to answer your questions, references at the end of the article.
Happy reading!😀
Have any questions, remarks, or experience to share? Feel free to use the comments section at the end of the article!🙏
Last updated: June 2024. Written by Juliet S diagnostic radiographer.
Disclaimer: no affiliate links.
Summary: Good diabetes management and regular foot care help prevent severe foot sores that are difficult to treat which may require foot amputation.
◀️Understanding the effect of diabetes mellitus and foot amputate.
When you have been diagnosed with diabetes it is very important to manage your diabetes and take care of your feet.
The connection between diabetes and serious foot problems might not seem obvious. And you might be wondering how these two are linked.
When does diabetes become a problem to your lower limb (feet)
Diabetes is a chronic, metabolic disease characterised by elevated levels of blood glucose or blood sugar, which leads over time to serious damage to the heart, blood vessels, eyes, kidneys, and nerves.
When you have diabetes mellitus, a disorder in which the body does not produce enough or respond normally to insulin causing blood sugar levels to be abnormally high.
This increases the risk of foot amputations.
▶️What causes foot amputation in diabetic patients?
Diabetes is linked to two conditions that raise the chances of foot amputation:
1️⃣Peripheral artery disease (PAD)
2️⃣Diabetic neuropathy.
What is diabetic a peripheral arterial disease?
Peripheral arterial disease (PAD) refers to partial or complete obstruction of the peripheral vessels of the upper and lower limbs.
By this I mean blood vessels in the legs become blocked or narrowed due to fat deposits which leads to reduced blood flow to the feet and legs.
Poor circulation then will make the skin on your feet and legs more prone to injury, infection, and ulceration.
Healing of skin that has been injured is slow and infection may spread. Pain in your legs may reduce your mobility.
The presence of diabetes mellitus greatly will increase the risk of Peripheral arterial disease (PAD) which could lead to feet amputation.
Diabetic neuropathy.
Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerves throughout the body.
Diabetic neuropathy most often damages nerves in the legs and feet where you will feel a loss of sensory function beginning distally in the feet, that is also characterised by pain and substantial morbidity.
Over time, at least 50% of individuals with diabetes develop diabetic neuropathy.
Feldman 2019
▶️What can you do to help prevent and manage peripheral and diabetic neuropathy from causing your foot to amputate?
Because of reduced blood flow, wounds may be slow to heal or not heal at all.
As a result, tissue can become damaged, and an infection can develop and spread to the bones.
Once this happens, amputation is often the only option.
To help prevent more damage.
Ideally, a multidisciplinary team approach, which involves a team of specialist such as:
Endocrinologist, a neurologist , nurses, podiatrists, psychologists, physical therapists, pain specialists, orthotists, orthopaedic surgeons, vascular surgeons, and microbiologists (when there is bacterial infection of an ulcer),
Are consulted to provide personalised and enhanced patient care.
Management of Diabetic sensorimotor peripheral neuropathy involves finding strategies aimed at the prevention of progression of DSPN and addressing foot complications such as.
🟤Neuropathic pain.
🟤 Comorbid mood disorders.
🟤Restlessness.
🟤Autonomic symptoms, unsteadiness, and falls.
Peripheral arterial disease (PAD) treatment is based around managing cardiovascular risk factors such as:
🟤Quitting smoking.
🟤keeping your HbA1c under 6.5%, lowering blood pressure and cholesterol.
🟤Exercises and minding your body weight.
The good news is that managing your diabetes and taking care of your feet can help prevent foot amputation.
When you get a foot ulcer, it’s important to get care immediately. Lower leg and foot amputations begin with foot ulcers.
An ulcer that won’t heal causes severe damage to tissues and bone. It may require surgical removal (amputation) of a toe, a foot or part of a leg.
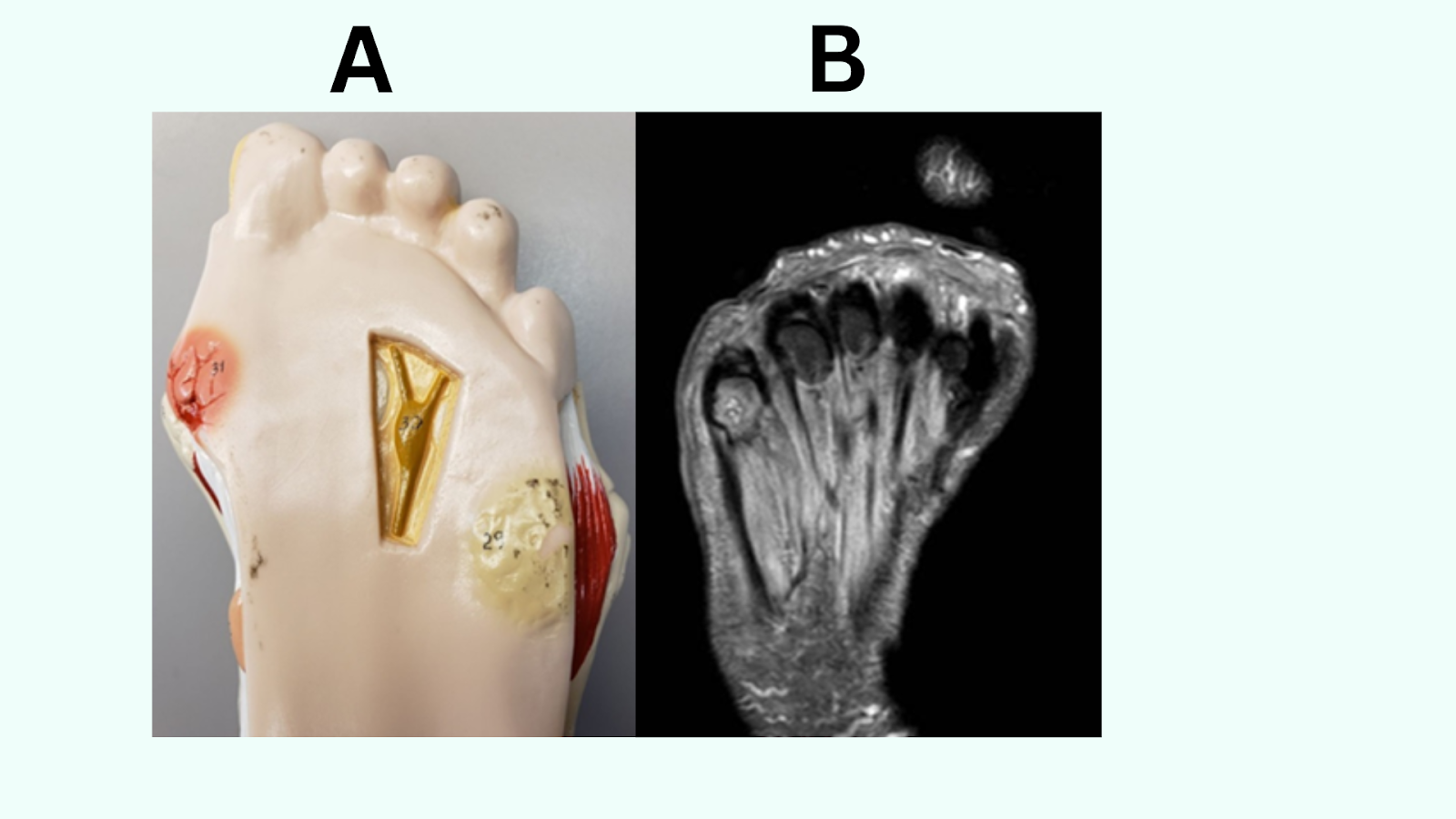
Image: A Diabetic foot model showing full-thickness ulceration & pre-ulcerative lesion: (B) MRI image of a patient with uncontrolled diabetes.(image: (Contributed by Aaron R).
And the main cause is diabetic peripheral arterial disease accelerated by the direct damage to the nerves and blood vessels.
Diabetic sensorimotor peripheral neuropathy (DSPN) develops insidiously. Most patients find them self-symptomless.
However, some patients experience varying combinations of symptoms, including:
🟣Numbness when you feel like your feet are dead with no feeling, paraesthesia, and neuropathic pain.
Painful symptoms include:
🟣A burning, ‘electric shock-type’, sharp, cold, and aching pain, Hyperalgesia (increased pain from a stimulus that norm and allodynia (pain due to a stimulus that does not normally provoke pain).
The intensity of neuropathic pain is typically worse at night, frequently causing insomnia.
Some patients report pain on weight bearing related to walking on pebbles or hot sand.
When you find yourself in such a state you will feel profoundly disabled, experience mood disorders, have a reduced quality of life and might struggle to maintain full employment.
When you have debates, you are usually told to monitor your blood sugar levels, blood pressure and cholesterol.
When these three components consistently become high, this can seriously damage the blood vessels in your feet.
You might be doing all that, but it is very important to:
▶️Understand the signs and symptoms of foot problems to help you act better.
Unfortunately, for many people, diabetic peripheral arterial disease does not present any symptoms. If symptoms do occur, they may include:
🟢Feeling numb or cold in the lower legs
🟢Pale or blue tinged legs
🟢Infections or sores on the feet or legs
🟢Hair loss on the legs or feet
🟢Extensive healing process.
Other Possible signs of foot problems that could be a cause of diabetes.
🟢Pain or Loss of feeling in your feet or legs could be a possible sign of a serious foot problem.
🟢Changes in colour (Blue) or shape of your skin foot
🟢Having a blister or cut that you can’t feel.
🟢Ingrown toenails
🟢Flesh-coloured bumps with dark specks (plantar warts) on the bottoms of your feet
🟢An open sore or bleeding, Swelling, Redness and Warmth in one area.
🟢A foul Smell
🟢An ulcer that lasts longer than 1 to 2 weeks
🟢An ulcer bigger than 3/4 inch (2 centimetres)
🟢A sore that doesn’t quickly begin to heal.
🟢An ulcer so deep you can see the bone underneath.
Caution!⚠️ These signs can happen very quickly for example a blister can turn into an amputation in less than a week. So, acting straight away is vital.
You can reduce your risk of an amputation by knowing the signs of serious foot problems and understanding what action to take if you spot one.
▶️What happens if you don’t amputate a leg in diabetes?
If you decide not to go through an amputate when your feet are affected by diabetes problems. This might cause:
Tissue in the leg to die due to lack of oxygen and nutrients, which leads to infection and gangrene.
In some cases, gangrene can be very dangerous as the infection can spread through the body and become life-threatening.
If the infection cannot be stopped or the damage cannot be reversed, amputation of your feet, toes or leg may be necessary.
Yes, I have seen patients refuse to get amputated. However, you might be at risk of severe infection, followed by the worsening of your condition, and severe pain.
I suggest that you discuss all potential outcomes and treatment options with your doctor so that you can make an informed decision.
▶️What happens when your foot is amputated?
Foot amputation is surgery to remove part or all your foot which will be done under anaesthesia so you will not feel pain.
Your doctor will leave as much healthy bone, skin, blood vessel, and nerve tissue as possible.
🟢 After a foot amputation, you will have bandages, a rigid dressing which will remain on for 3 or more days, or a cast over the remaining part of your leg or foot.
🟢You may have pain for the first few days. You will be able to take pain medicine as you need them.
🟢You may have a tube that drains fluid from the wound. This will be taken out after a few days.
▶️Recovering from a Diabetic amputation of the foot.
Recovery after a diabetic foot amputation can take longer and be more challenging than recovery from other types of amputations.
Diabetes can impede blood flow to the feet and lower extremities leading to slower wound healing.
🟩During the initial recovery period, you will need to rest and keep your amputated limb elevated to reduce swelling.
🟩Take your medications to manage pain and prevent infection.
🟩Physical therapy will begin soon after the surgery to help you regain strength, mobility, and the ability to perform transfers.
Physical rehabilitation is an important part of the recovery process.
After rehabilitation, you should be able to return to work and other activities.
| Phases | Timeline |
| Your leg or foot after surgery may be swollen for- | 4 weeks or longer |
| Pain or feeling in the remaining part of your foot after surgery which is called phantom pain is common. | It may come and go for one year. |
| A bandage or rigid dressing cast- non weight bearing on the affected foot until the wound has healed | The wound will be checked daily for inflammation and swelling, and the dressing is changed every day by a home nurse. |
| Walking and standing will be more difficult for you at first-you will use walking aids for some time. | A few months until you start using your prosthetic foot shoe. |
| for your wound to heal completely. | 4 to 6 weeks If the site heals well and there are no complications, you can begin to use your prosthetic. Healing can take 8 weeks or more. |
▶️How can you avoid amputations when you have diabetes?
Good diabetes management and regular foot care helps prevent severe foot sores that are difficult to treat and may require amputation.
Diabetes complications can include nerve damage and poor blood circulation. These problems can lead to skin sores (ulcers) on the feet that can get worse quickly.
The good news is that managing your diabetes and taking care of your feet can help prevent foot ulcers.
Here’s how to keep your feet healthy.
1️⃣Preventing foot ulcers
The best way to prevent complications of diabetes including foot ulcers is to manage your diabetes.
You should try to eat a healthy diet, exercising regularly, checking your blood sugar regularly and taking your medicine correctly.
2️⃣Proper foot care includes the following:
⏭️Check your feet once a day for blisters, cuts, cracks, sores, redness, tenderness or swelling.
If you have trouble reaching your feet, use a hand mirror to see the bottoms of your feet. Put the mirror on the floor if you can’t hold it or ask someone to help you.
⏭️Wash your feet every day. Wash your feet in lukewarm (not hot) water once a day. Dry them gently, especially between the toes. Use a pumice stone to gently rub the skin where calluses easily form.
Put talcum powder or corn-starch between your toes to keep the skin dry.
You can use a moisturising cream or lotion on the tops and bottoms of your feet to keep the skin soft. Preventing cracks in dry skin helps keep bacteria from getting in.
⏭️Don’t remove calluses or other foot lesions yourself. To avoid hurting your skin, don’t use a nail file, nail clipper or scissors on calluses, corns, or warts.
Don’t use chemical wart removers! Seek medical advice.
⏭️Cut your toenails carefully. Cut your nails straight across. Carefully file sharp ends with a nail file board. Ask someone for help if you can’t trim your nails yourself.
⏭️Avoid walking barefoot even around the house to keep from hurting your feet.
⏭️Wear clean and dry socks made of material that pulls sweat away from your skin. This includes cotton and special acrylic fibres but not nylon.
Don’t wear socks with tight elastic bands because these bands reduce circulation.
⏭️Buy shoes that fit correctly are comfortable and provide support and cushioning for the heel, arch, and ball of the foot.
Avoid tightfitting shoes and high heels or narrow shoes that crowd your toes.
Your doctor may recommend specially designed orthopaedic shoes. These shoes fit the exact shape of your feet, cushion your feet, and make sure your weight is the same on both feet.
⏭️Stop or reduce smoking because it makes it harder for your blood to go through your body. It also reduces the amount of oxygen in your blood.
These problems can make wounds worse and slow down healing. Talk to your provider if you need help quitting smoking.
⏭️Schedule regular foot check-up’s. Your podiatrist can look at your feet for signs of nerve damage, poor circulation, or other foot problems. Having a foot exam at least once a year or more is very important.
We have come to the end of this article, any questions, let’s meet in the comments section.
Take care of your foot, Wishing you a quick recovery!🙋
📚Sources:
Thiruvoipati T, Kielhorn CE, Armstrong EJ. Peripheral artery disease in patients with diabetes: Epidemiology, mechanisms, and outcomes. World J Diabetes 2015; 6(7): 961-969 [PMID: 26185603 DOI: 10.4239/wjd.v6.i7.961]
Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW, Wright DE, Bennett DL, Bril V, Russell JW, Viswanathan V. Diabetic neuropathy. Nat Rev Dis Primers. 2019 Jun 13;5(1):42. doi: 10.1038/s41572-019-0097-9. PMID: 31197183; PMCID: PMC7096070.
Ward, J. D. The diabetic leg. Diabetologia 22, 141–147 (1982).
Sloan, G. et al. A new look at painful diabetic neuropathy. Diabetes Res. Clin. Pract. 144, 177–191 (2018)
Tesfaye, S., Boulton, A. J. & Dickenson, A. H. Mechanisms and management of diabetic painful distal symmetrical polyneuropathy. Diabetes Care 36, 2456–2465 (2013)
Kayla Song; Aaron R. Chambers. Treasure Island (FL): StatPearls Publishing; 2024 Jan-