
Frozen shoulder is one of the annoying pathologies very often I see in radiology. It is a condition that limits movement in the shoulder joint. You usually have pain and stiffness that comes on gradually, gets worse, and then finally goes away.
Have you been diagnosed with adhesive capsulitis and are you looking for a simple and comprehensive guide on what to do to help with your pain.
Drawing from my experience as a diagnostic radiographer and my research in medical studies I will answer some of the frequently asked questions from patients who have been diagnosed.
Happy reading!😀
Any questions? remarks? Let’s meet in the comments section at the end of this article.🙏
Last updated: Sept 2024. Written by Juliet Semakula, a diagnostic radiographer.
▶️What exactly is a frozen shoulder (Adhesive capsulitis).
There are so many medical terms that have been used to describe Adhesive capsulitis such as.
o frozen shoulder
o Periarthritis of the shoulder,
o Tendinitis of the short rotators.
o Periarthritis scapulae
All these in medical terms mean the same thing: Adhesive capsulitis which is a common shoulder condition characterised by pain and decreased range of motion, especially in external rotation.
Frozen shoulder is a condition that can result in a painful and stiff shoulder. Within the shoulder joint there is a capsule that is normally elastic, thus allowing the shoulder to move freely.
With a frozen shoulder this normally elastic capsule becomes contracted, causing pain and stiffness as a result.
▶️How can you be sure that you have a frozen shoulder?
You can only be sure when you have gone to the doctor and an assessment is done usually following these three elements.
1️⃣Your medical history.
2️⃣You will have a clinical examination to assess the symptoms you may be having.
3️⃣One or more imaging tests.
The onset of symptoms tends to be more gradual than in other shoulder conditions.
Physical examination does not reveal a specific point of tenderness. Occasionally, the long head of the biceps tendon is tender because its synovium is confluent with that of the glenohumeral joint.
⚠️Caution!⚠️ When you have pain following repetitive overhead activity, you should know it is not a typical feature of a frozen shoulder and is suggestive of other pathology such as osteoarthritis of the shoulder, tendinitis and cervical brachial neuralgia.
▶️Here are the main symptoms:
🟠Shoulder pain
Usually when you have shoulder pain accompanied by a marked decrease in range of motion, This is the chief characteristic of adhesive capsulitis.
Pain is described as a poorly localised, dull ache, and may radiate into the biceps. Reaching overhead or behind the back may stimulate the sensation of pain and stiffness.
Night pain is common, and it can distract your sleep, and you may not be able to lay on the affected side.
🟠Loss of motion
You may find it difficulty dressing, combing your hair, reaching to a back pocket, or fastening a brassiere.
Pain is reduced and may be apparent only when the shoulder is moved beyond the limits allowed by the contracted capsule.
🟠Associated neck pain when you try to move your head.
⚠️Caution!⚠️ Symptoms such as fever, night sweats, malaise, or unexplained weight loss should prompt the physician to consider an alternative diagnosis such as neoplasm or an autoimmune disease.
Diagnosis tests.
Although imaging is not necessary to make the diagnosis, a finding of coracohumeral ligament thickening on non-contrast magnetic resonance imaging (MRI) yields high specificity for adhesive capsulitis
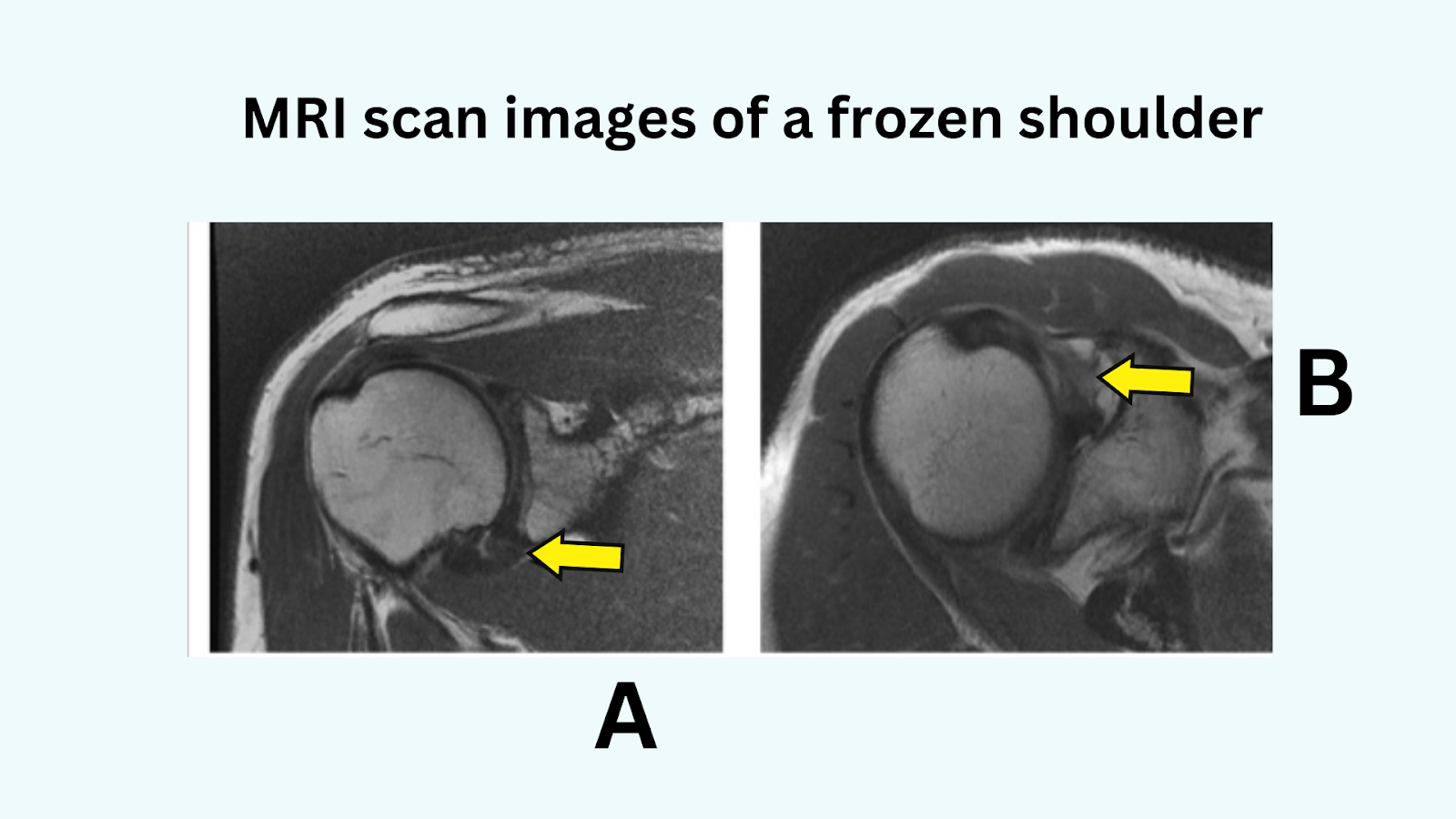
An MRI scan showing images demonstrating thickening of the dependent portion of the capsule arrow A and scarring of the rotator interval arrow B.
It is recommended that x-ray is ordered to rule out osseous pathology and evaluate other shoulder problems such as arthropathy or calcific tendonitis.
▶️What are the 4 stages of frozen shoulder?
Adhesive capsulitis is often self-limited; however, it can persist for years with some patients never regaining full function of their shoulder
The four stages of a frozen shoulder have been described based on the arthroscopic appearance of the joint capsule.
Stage 1️⃣: The pre-adhesive stage, consists of a fibrinous inflammatory synovitis reaction without adhesion formation
At this stage, you will typically have full motion but report pain, particularly at night. Symptoms are nonspecific, and misdiagnosis is common.
Stage 2️⃣: An acute adhesive synovitis with proliferation of the synovium and early formation of adhesions.
Pain is a prominent feature, and motion loss is present but typically mild
Stage3️⃣: The maturation stage involves less synovitis and more fibrosis.
Here you will feel pain less severe than in stages 1 and 2, but motion is significantly restricted.
Stage 4️⃣: The chronic stage, adhesions are fully mature, and motion is severely reduced.
At this stage you may have painless, limited range of motion, but pain may occur when the arm is suddenly moved beyond the limits of the scarred capsule.
▶️What is the root cause of a frozen shoulder?
The natural history of the causes of adhesive capsulitis remains a matter of debate.
Although experts don’t always agree, the most accepted cause of frozen shoulder is inflammation of the tissues around the shoulder joint.
♦️Inflammation within the shoulder capsule joint.
The capsule of the shoulder joint has ligaments that hold the shoulder bones to each other.
When the capsule becomes inflamed this is called rotator cuff tendinitis where inflammation of the bursa, small slippery fluid filled sacs that the tendons glide over.
This causes a frozen shoulder because the shoulder bones are unable to move freely in the joint.
♦️The shoulder joint which is enclosed in a capsule of connective tissue makes the capsule thicken and tighten around the shoulder joint, restricting its movement.
This usually happens after keeping your shoulder still for a long period after an arm injury, stroke, a rotator cuff or fracture and surgery.
▶️Why do some people have more frozen shoulder issues?
It is not yet clear why some people develop frozen shoulders and others do not.
However certain factors and disease are found more often to increase the risk of developing a frozen shoulder.
🟢 Age factor 40 and above especially women are more likely to have frozen a shoulder.
🟢Cardiovascular disease
🟢Thyroid dysfunction.
🟢 Breast cancer treatment.
🟢Myocardial infarction
🟢Cerebrovascular accident
🟢Parkinson’s disease.
🟢Diabetes mellitus and hypothyroidism.
A meta-analysis found that patients with diabetes were five times more likely than the control group to have adhesive capsulitis (Zreik 2016)
▶️What is the possible management or treatment? How do you unfreeze a frozen shoulder?
The most effective treatment for adhesive capsulitis is uncertain.
Nonsurgical treatments include:
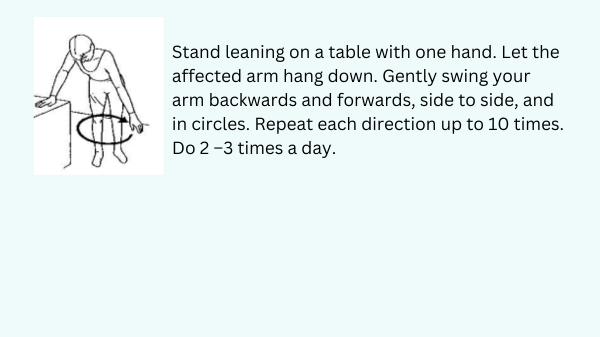
1️⃣Physiotherapy and rehabilitation Frozen shoulder exercises
Physiotherapy has traditionally been used to treat adhesive capsulitis despite a lack of high-level studies demonstrating benefit over observation or medical therapy alone.
Physical therapy combined with a home exercise program regardless of stage.
Therapy using manual mobilisation techniques with exercise provides an increased range of motion and function for frozen shoulder issues.
Therapy need not be aggressive or painful, and strengthening is rarely necessary.
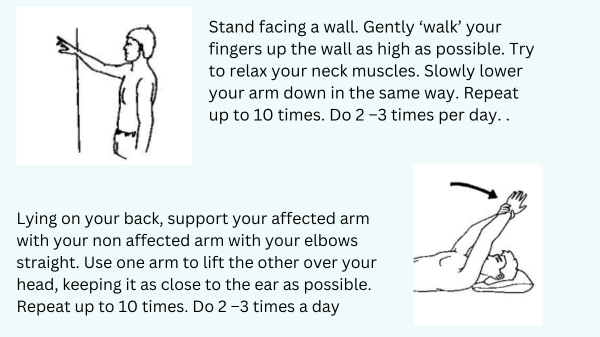
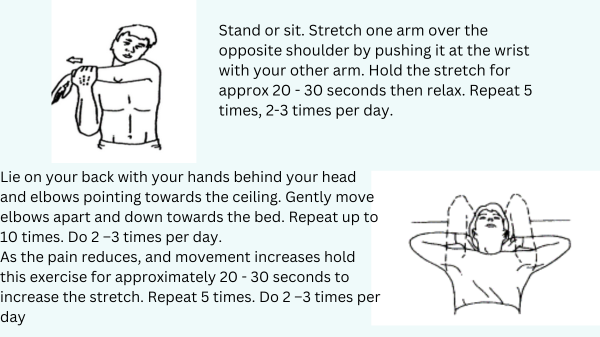
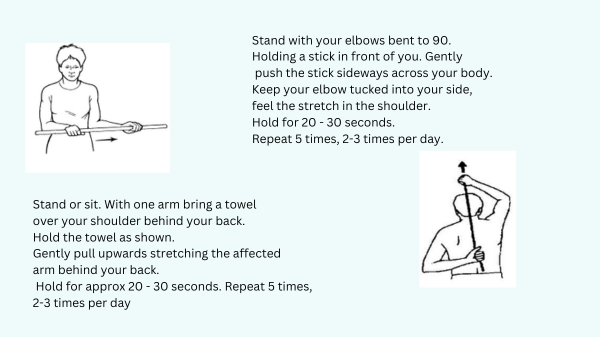
Gentle progressive stretching is optimal and is effective in most cases.
The number of physical therapy sessions varies case by case. Here are some of the stretching exercises for a frozen shoulder.
2️⃣Medical treatment options: Medication and injections
You may be given nonsteroidal anti-inflammatory drugs such as:
♦️️ Nonsteroidal anti-inflammatory drugs such as (NSAIDs) are often prescribed for pain relief.
However, there is little evidence for their effectiveness in treating adhesive capsulitis specifically.
♦️Oral corticosteroid.
A review from a medical study, concluded that oral corticosteroids may produce a small short-term benefit (less than six weeks) in pain relief and improved range of motion, but it was not maintained in the long-term (Buchbinder 2006).
Some medical studies suggest that given the risks associated with extended oral corticosteroid usage, and the lack of long-term benefit, oral corticosteroids should not be used routinely to treat adhesive capsulitis.
♦️Intra-articular corticosteroid injections
Evidence suggests that intra-articular corticosteroid injections are more effective than placebo for pain relief in the short-term, but results vary in the long-term
♦️Acupuncture.
♦️ Hydro dilatation.
Hydro-dilatation (arthroscopic distension) involves an injection of local anaesthetic into the shoulder capsule at high pressure to distend and stretch the joint capsule.
A randomised controlled study of 46 patients compared hydro-dilatation with placebo and demonstrated statistically and clinically significant improvement in functional outcome scores at six weeks following intervention.
Physiotherapy and corticosteroid injections combined may provide greater improvement than physiotherapy alone
3️⃣Apply a cold pack of ice or frozen peas wrapped in a damp towel. This can provide short-term pain relief.
Apply this to the sore area for up to 15 minutes, every three hours and up to four times a day, ensuring the ice is never in direct contact with the skin.
4️⃣Relative rest: reduce activities that are making your symptoms worse, for example, the duration of time you spend on your feet.
5️⃣Surgical treatment options for patients who have minimal improvement after 6 to 12 weeks of nonsurgical treatment include:
♦️Manipulation under anaesthesia.
Manipulation is a technique performed under general anaesthesia where the humerus is manipulated to disrupt adhesions
Moderate evidence suggests that manipulation alleviates pain and can improve range of motion when followed by early physiotherapy
♦️Arthroscopic capsular release.
▶️How does frozen shoulder naturally progress?
Studies that track the progression of patients diagnosed with frozen shoulders, plus those who decide not to get any medical or physiotherapy treatment.
Some of these studies point out:
🔴Some people after 1 to 4 years of follow-up, they notice shoulder range of motion improving but not fully return to normal in most people.
🔴within the first few weeks or months symptoms of a frozen shoulder show a big improvement relatively.
🔴In a group of 83 people, recovery was declared on average 15 months after the onset of symptoms.
🔴More than half of the people no longer felt any pain during activity, at rest, or at night, and 9 out of 10 had resting pain rated below 3/10.
Source: Wong 2017, Vastamäki 2012
We have come to the end of this article, any questions lets meet in the comments section. Wishing you a quick recovery 🙋
📚Sources:
Ramirez J. Adhesive Capsulitis: Diagnosis and Management. Am Fam Physician. 2019 Mar 1;99(5):297-300. PMID: 30811157.
Zreik NH, Malik RA, Charalambous CP. Adhesive capsulitis of the shoulder and diabetes: a meta-analysis of prevalence. Muscles Ligaments Tendons J. 2016 May 19;6(1):26-34. doi: 10.11138/mltj/2016.6.1.026. PMID: 27331029; PMCID: PMC4915459.
Buchbinder R, Green S, Youd JM, Johnston RV. Oral steroids for adhesive capsulitis. Cochrane Database Syst Rev. 2006 Oct 18;2006(4):CD006189. doi: 10.1002/14651858.CD006189. PMID: 17054278; PMCID: PMC8919374.
Chi AS, Kim J, Long SS, Morrison WB, Zoga AC. Non-contrast MRI diagnosis of adhesive capsulitis of the shoulder. Clin Imaging. 2017;44: 46-50.
Buchbinder R, Green S, Forbes A, Hall S, Lawler G. Arthrographic joint distention with saline and steroid improves function and reduces pain in patients with painful stiff shoulder: results of a randomized, double blind, placebo-controlled trial. Ann Rheum Dis. 2004;63(3):302-309.
Wise SR, Seales P, Houser AP, Weber CB. Frozen Shoulder: Diagnosis and Management. Curr Sports Med Rep. 2023 Sep 1;22(9):307-312. doi: 10.1249/JSR.0000000000001097. PMID: 37678349.
Redler LH, Dennis ER. Treatment of Adhesive Capsulitis of the Shoulder. J Am Acad Orthop Surg. 2019 Jun 15;27(12):e544-e554. doi: 10.5435/JAAOS-D-17-00606. PMID: 30632986.
Wong CK, Levine WN, Deo K, Kesting RS, Mercer EA, Schram GA, Strang BL. Natural history of frozen shoulder: fact or fiction? A systematic review. Physiotherapy. 2017 Mar;103(1):40-47. doi: 10.1016/j.physio.2016.05.009. Epub 2016 Jun 21. PMID: 27641499.
Vastamäki H, Kettunen J, Vastamäki M. The natural history of idiopathic frozen shoulder: a 2- to 27-year followup study. Clin Orthop Relat Res. 2012 Apr;470(4):1133-43. doi: 10.1007/s11999-011-2176-4. Epub 2011 Nov 17. PMID: 22090356; PMCID: PMC3293960.