
Has your child been diagnosed with Osteogenesis imperfecta disease. Are you wondering if a child with the disease will be able to live a normal life.
Osteogenesis imperfecta has been a topic of interest for basic scientists and a source of frustration to clinicians.
However, much progress has been made concerning the treatment and care. so rest be assured your child will be able to leave a decent life if well supported with the available treatments.
Summary: People with Osteogenesis imperfecta can live a normal life because different treatments have been clinically proven to allow people with the disease to function as independently as possible as they get older.
So here I am writing this article based on two things.
⚪My knowledge and experience as a diagnostic radiographer.
⚪ My documentary research in the international medical studies.
Happy reading!😃
Any questions? remarks? Let’s meet in the comments section at the end of this article.🙏
Last updated: Oct 2024. Written by Juliet Semakula a diagnostic radiographer
Disclaimer: no affiliate links.
▶️Why do some people have Osteogenesis imperfecta and others do not?
What is Osteogenesis imperfecta and what causes it.
Osteogenesis imperfecta is a genetic or heritable disease in which bones fracture (break) easily, often with no obvious cause or minimal injury.
Our bones have type 1 collagen, a material in bones that helps make them strong.
But when there is a change or defect in the gene that carries the instructions for making type 1 collagen then the defect in the genes.
This causes the body to make incorrect collagen leading to weak and brittle bones and other connective-tissue signs in which the body is unable to form healthy bones.
Mutations in several genes can lead to Osteogenesis imperfecta. About 80%–90% of OI cases are caused by autosomal dominant mutations in the type 1 collagen genes, COL1A1 and COL1A2. Mutations in one or the other of these genes cause the body to make either abnormally formed collagen or too little collagen.
Your child will be bone with Osteogenesis imperfecta, Hence at this point there is no cure of the disease.
▶️ At what age is osteogenesis imperfecta diagnosed?
Osteogenesis imperfecta is usually diagnosed during prenatal ultrasound at 18 to 24 weeks of pregnancy.
If a parent or sibling has OI, the DNA of the foetus will be tested for the presence of an OI mutation.
The disease can also be diagnosed by X-ray, CT-scan, blood tests and physical examination after you give birth.
▶️What are the different types of Osteogenesis imperfecta
The type and severity of the disease is classified from mildest to severe.
Here is a table showing an overview of the major types that are often diagnosed.
| Type I | Most severe type among those who survive the neonatal period and usually results in the greatest number of physical disabilities. Easily broken bones with very little trauma over a lifetime. Moderate to severe bone deformity. Small stature and loose joints Blue, purple, or grey tint to sclera. Poor muscle development in arms and legs. Barrel-shaped rib cage and Triangular face. Curved spine and compression or collapse of vertebrae. Possible lung problems that worsen with age. Often severe bone deformity. Possible changes to the strength and colour of teeth with tooth fracture. Possible malocclusion of the teeth, meaning they are not aligned properly. Possible changes to the strength and colour of teeth. Possible hearing loss. Improperly formed collagen. |
| Type II | Causes death at birth or shortly after, because of the inability to breathe.Numerous broken bones that develop before birth while the baby is still in the womb.Severe bone deformities.Very small stature.Underdeveloped lungs.Blue, purple, or Gray tint to sclera.Improperly formed collagen. |
| Type III | Most severe type among those who survive the neonatal period and usually results in the greatest number of physical disabilities.Easily broken bones with very little trauma over a lifetime. (Broken bones are often present at birth, and x-rays may reveal healed bone breaks that occurred before birth.)Moderate to severe bone deformity.Small stature.Blue, purple, or grey tint to sclera.Loose joints.Poor muscle development in arms and legs.Barrel-shaped rib cage.Triangular face.Curved spine and compression or collapse of vertebrae.Possible lung problems that worsen with age.Often severe bone deformity.Possible changes to the strength and colour of teeth with tooth fracture.Possible malocclusion of the teeth, meaning they are not aligned properly.Possible changes to the strength and colour of teeth.Possible hearing loss.Improperly formed collagen. |
| Type IV | Bones break easily, sometimes before birth, with most broken bones occurring before puberty.Smaller than average stature.White or blue tint to sclera.Mild bone deformity.Vertebra compression or collapse.Barrel-shaped rib cage.Triangular face.Possible changes to strength and colour of teeth.Possible hearing loss.Improperly formed collagen. |
| Type V | Clinically like Type IV OI in appearance and symptoms.A dense band seen on x-rays by the cartilage growth plate of the long bones.Unusually large calluses, called hypertrophic calluses, at the sites of fractures or surgical procedures. (A callus is an area of new bone that is laid down at the fracture site as part of the healing process.)Calcification of the membrane between the radius and ulna (the bones of the forearm), which results in restricted arm movement.Possible loose joints.White sclera.No changes to teeth.“Mesh-like” appearance to bone when viewed under the microscope.Changes in the mineralization of bone. |
| Type VI | Resembles Type IV OI in appearance and symptoms.Not always diagnosed at birth, and symptoms progress over time.“Fish-scale” appearance to bone when viewed under the microscope.Curved spine.Diagnosed by bone biopsy or genetic studies.Changes in the mineralization of bone. |
| Type VII | Resembles Type II and Type III OI in appearance and symptoms. |
| Type VIII | Resembles Type II and Type III OI in appearance and symptoms. |
Retrieved from (Marom 2020) Osteogenesis imperfecta
▶️ Can you prevent or cure osteogenesis imperfecta?
To date, there is no known treatment, medicine, or surgery that will cure osteogenesis imperfecta (OI).
Anyone can be born with Osteogenesis imperfection, if you have a family history of the disease you will be at a greater risk of inheriting it through an abnormal gene that is passed on from one or both parents.
The only way you can try to avoid having a child with the disease is to have a genetic test done before you start a family.
This will help you make a decision whether to go ahead or find someone else with different genes.
▶️What are some of the symptoms of Osteogenesis imperfecta
All people with the disease have weak, brittle bones. Some people may have only a few broken bones over their lifetime.
Others may have hundreds of broken bones in their lifetime, including broken bones that occur before birth.
Other symptoms that can range from mild to severe and vary from person to person are:
🟢 Malformed or bowing of long bones.
🟢Small stature and Skin that bruises easily.
🟢 Loose joints and Weak muscles.
🟢 Whites of the eyes (sclera) that look blue, purple, or grey.
🟢 A face shaped like a triangle.
🟢 A rib cage shaped like a barrel. And a curved spine.
🟢Collapse or compression of the vertebrae in the spine.
🟢Brittle, misshapen, or discoloured teeth.
🟢Malocclusion of teeth, meaning they are not aligned properly.
🟢Hearing loss and Breathing problems.
🟢A deformed hip joint in which the neck of the femur is bent downward, a condition called coxa Vara.
🟢Joint contractures (a joint stays in a permanently bent or straightened position).

▶️ What treatment and management should be implemented for Osteogenesis imperfecta?
There are several studies over the years that examine different treatments and their outcome on the disease.
That’s why for this part I also rely on the results of these studies to discuss the available treatments and management of Osteogenesis imperfecta disease.
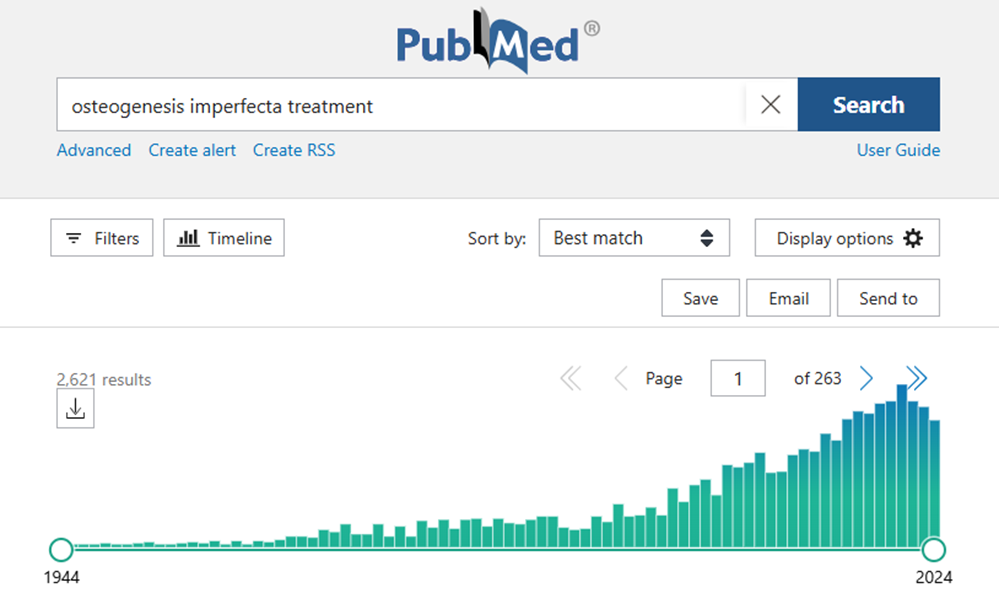
Here is the number of scientific publications on the treatment of Osteogenesis imperfecta disease.
There are many factors that come into play when deciding what treatment to adopt in the case of Osteogenesis imperfecta disease.
In particular, the extent severity, type, age and functional status of patients:
The main goal of treatment is to prevent deformities and fractures and allow you to function as independently as possible as you get older.
A multi-disciplinary approach is used to address not only the fractures, reduced mobility, growth and bone pain but also other extra-skeletal manifestations
A team of medical specialists which includes an orthopaedic surgeon, endocrinologist, pulmonologist, neurologist, surgeon, radiologist, dentists, and nutritionist, are needed to deliver excellent care.
Treatments for preventing or correcting symptoms may be given based on how severe, mild or moderate the disease is.
1️⃣Conservative treatment
If your child has a mild symptom of the disease, there will be subtle restriction put in place such as:
Pharmacological approaches:
The use of bisphosphonates therapy is considered the gold standard in increasing bone mineral density in children and adults with this condition. And a reduction in fracture rates and bone pain is noticed (Dwan 2016)
Treatment with Denosumab has been shown to improve bone mineral density in patients with OI type VI who do not respond well to bisphosphonate therapy in a few small-scale studies (Hoyer-Kuhn,2014)
Medical therapies such as growth hormone
Small studies have suggested that growth hormone treatment may accelerate short-term height velocity in some patients. (Glorieux 2008)
However, some studies suggest that growth hormone treatment appears to be less efficient in the more severe OI type III. There is not enough data to support its benefit in the treatment of OI, and currently this approach is not in standard clinical use.
2️⃣Physiotherapy rehabilitation
You will have a physiotherapist to help with your rehabilitation. These sessions are mainly strengthening exercises that focus on stretching, bracing and functional activities etc.
Physical activity programmes are encouraged to prevent contractures and immobility-induced bone loss
3️⃣Surgical option to correct any fractures caused by the deformity.
Severe deformities and fractures usually in the midshaft tibial are managed by open reduction and internal fixation with plate osteosynthesis and referred to physiotherapy.
Here an intramedullary rod with osteotomy used to correct severe bowing of long bones.

An 8-year-old female with osteogenesis imperfecta had severe anterior bowing of the tibia and recurrent fractures (A). This case failed nonoperative management with a brace. The patient underwent a 2-level open tibial osteotomy with placement of a telescoping rod (B). The patient is now over 1 year out from surgery. Note the increased growth and telescoping of the rod (C – red arrow). The osteotomies have healed well, and the patient is currently asymptomatic (Marom,2020)
Standing and walking can often only be achieved after femora and tibia have been straightened using intramedullary rods
▶️The Role of Physical and Occupational Therapy in Managing Osteogenesis imperfecta
🔴To listen to individuals with the disease and their families because they are the experts on how OI affects them.
🔴To set personal goals that are achievable on how they are going to live a normal life.
🔴Guidelines on how to reduce fractures because it is common with the disease.
🔴To help with weakness because it is a significant constraint to movement in OI
Physical therapy rehabilitation
Physiotherapy plays one of the important roles in the management of Osteogenesis imperfecta along with medical and orthopaedic management.
Therapeutic interventions: the goal of treatment for osteogenesis imperfecta is to decrease pain and fracture risk while promoting mobility.
Physical therapy involves strengthening exercises to strengthen the upper limb and lower limb muscles.
The physical therapist will follow a developmental sequence, beginning with head and trunk control, seated balance, and walking.
Protective handing to help with skill development
Some children might not be able to crawl but may develop other methods of floor mobility such as snaking or bottom scooting.
A skate or scooter board can be used to eliminate the pull of gravity and encourage mobility.
Introduce new positions and skills gradually to allow the person to feel safe as well as to promote gradual strengthening of muscles and bones.
The aim is to provide adequate support to overcome weakness and prevent injury
Protective handling during stretching exercises.
You must have extensive knowledge of what handling practices are safe for their individual children during therapy.
Never pull, push, or twist a limb. Be very cautious with any passive rotation of the arms, legs, head or trunk. Always encourage the family to let the child with OI assist with any of the positioning activities.
Mobility and active movement
Older adults may need therapy to learn how to effectively use walkers or canes after years of unassisted mobility.
Many people with OI use a mobility aid at some point in their lives or for certain situations. Some may only need assistance when they are learning a new skill or recovering from a fracture or surgery.
Some will use a walker, crutches, wheelchair, or other aid most of the time, while outdoors.
Bracing and splints, positioning aids
Braces should be used only if necessary to support weak muscles and should be lightweight.
To promote recline position in car seat, highchair, wheelchair, stroller rather than “frog leg” position, Pillows, bolsters, towel rolls, swim noodles, gel pads, etc. can be used for support.
Encourage healthy living by eating healthy and taking manageable physical activities to avoid obesity and other health problems that can put constraints on the bones and body.
▶️What are some of the strategies: Exercise and Fitness for Teens and Adults with Osteogenesis imperfecta
The treatment plan for an adult includes exercise and active recreation activities. And this is based on your interest, goals, preference, health history and precautions.
Medical clearance should be acquired with all new exercise routines.
Exercise Guidelines:
Having “Less is More” when initiating an exercise program is very important.
🟡Exercises should be performed in a slow and controlled manner with, focus on posture, form, and repetitions rather than increasing resistance.
🟡 Use joint protection techniques with all movements and equipment with awareness of posture and body alignment. For joint protection.
🟡 All movements should include trunk and core stabilisation
🟡Encourage proper alignment, posture, and body mechanics with all movements and exercises.
🟡Monitor tolerance to exercise with a goal of a total of 60 minutes per day of activity. Adults should monitor their tolerance to activity for integration into community based daily exercise routines.
🟡Choose activities that you enjoy and are meaningful for example swimming, upper body ergometer, walking, or cycling
When exercising in water, be conscious of the velocity of movement. Due to the degree of fragility, start with slow velocity and progress up from there but always be moving through the full available range of motion.
🟡Strength Training, including weight bearing activities on land and in water, improves bone density, triceps, and biceps muscles.
Safety and joint protection are very important during any kind of exercise. Always consider the risk level of any activity before you decide to participate.
People with OI can get more tired and experience more aches and pains compared to their peers. It is important to have rest breaks during activities and not over doing things will help.
There are some exercises that are not recommended for adults and children with the disease for example trampolining, contact sports that involve unpredictable collisions or falls.
▶️What are the long-term effects of osteogenesis imperfecta?
OI is a lifelong condition that varies greatly in severity, affecting bone quality and bone mass.
The condition can also affect a child’s stature, hearing, skin, blood vessels, muscle mass (hypotonia, or poor muscle tone), and teeth (dentinogenesis imperfecta).
What to remember: Osteogenesis imperfecta is a condition that can be managed with different treatment option to allow a decent function in many or most areas of daily life
We have come to the end of this article! Wishing you a quick recovery.🙋
Any questions or comments? Let me know in the comments!
📚Sources:
Deguchi M, Tsuji S, Katsura D, Kasahara K, Kimura F, Murakami T. Current Overview of Osteogenesis Imperfecta. Medicina (Kaunas). 2021 May 10;57(5):464. doi: 10.3390/medicina57050464. PMID: 34068551; PMCID: PMC8151368.
Glorieux FH. Osteogenesis imperfecta. Best Pract Res Clin Rheumatol. 2008 Mar;22(1):85-100. doi: 10.1016/j.berh.2007.12.012. PMID: 18328983.
Marom R, Rabenhorst BM, Morello R. Osteogenesis imperfecta: an update on clinical features and therapies. Eur J Endocrinol. 2020 Oct;183(4):R95-R106. doi: 10.1530/EJE-20-0299. PMID: 32621590; PMCID: PMC7694877.
Nangliya RM, Jain DS, Saklecha AV, Patil DS. Effect of physiotherapy rehabilitation on osteogenesis imperfecta with a midshaft tibial fracture in the 11-year-old patient: a case report. Pan Afr Med J. 2022 Dec 22;43:201. doi: 10.11604/pamj.2022.43.201.34702. PMID: 36942134; PMCID: PMC10024562.
Forlino A, Cabral WA, Barnes AM, Marini JC. New perspectives on osteogenesis imperfecta. Nat Rev Endocrinol. 2011 Jun 14;7(9):540-57. doi: 10.1038/nrendo.2011.81. PMID: 21670757; PMCID: PMC3443407.
Rossi V, Lee B, Marom R. Osteogenesis imperfecta: advancements in genetics and treatment. Curr Opin Pediatr. 2019 Dec;31(6):708-715. doi: 10.1097/MOP.0000000000000813. PMID: 31693577; PMCID: PMC7017716.
Dwan K, Phillipi CA, Steiner RD, Basel D. Bisphosphonate therapy for osteogenesis imperfecta. Cochrane Database Syst Rev. 2014 Jul 23;(7):CD005088. doi: 10.1002/14651858.CD005088.pub3. Update in: Cochrane Database Syst Rev. 2016 Oct 19;10:CD005088. doi: 10.1002/14651858.CD005088.pub4. PMID: 25054949.
Hoyer-Kuhn H, Netzer C, Koerber F, Schoenau E, Semler O. Two years’ experience with denosumab for children with osteogenesis imperfecta type VI. Orphanet J Rare Dis. 2014 Sep 26;9:145. doi: 10.1186/s13023-014-0145-1. PMID: 25257953; PMCID: PMC4180531.