
Do you or an elderly person in your circle have a pelvic fracture? You likely have many questions about treatment, rehabilitation and recovery time after a fractured pelvis.
As a diagnostic radiographer, I see so many fractured pelvis and for this reason I rely on my knowledge and scientific publications to try to answer your questions.
Happy reading!😀
▶️What are the different types of pelvic fractures in the elderly.
Pelvic fracture is a break in one or more bones in your pelvic. These are rare fractures that can range from mild to severe.
Pelvic fractures occur in 3% to 8% of trauma patients with a mortality of 5% to 14% (Baker,2023)
Over the years of my practice as a radiographer I have seen more of these fractures in the elderly.
So, for that reason I will focus more on the treatment and rehabilitation of pelvic fractures in the elderly.
▶️Basic anatomy of a pelvic.
The pelvis is located below the abdomen between the hip bone.it is made up of the sacrum, coccyx and hip bones that include ilium, ischium and pubis.
Together these bones make up the pelvic ring which is highly stable which protects your nerves, blood vessels, bladder and leg muscles.
Image of the pelvic bone
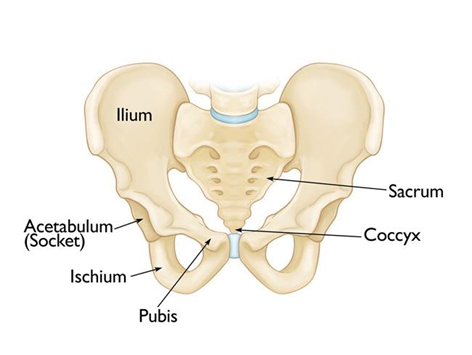
Image from:orthoinfo.aaos
▶️Different types of pelvic fractures in the elderly:
These Injuries of the pelvic ring are rare fractures compared with all other fractures. Most of these fractures I have seen in elderly women over the age of 60.
Here are the most common types of pelvic fractures
🟠Iliac wing fracture:
🟠Sacrum fracture
🟠Superior pubic ramus fracture
🟠Inferior pubic ramus fracture
Other terms used include:
🟠Pubic rami fracture
🟠Pelvic ring fracture
🟠Acetabular fracture
🟠Sacroiliac fracture
🟠ilioischial fracture
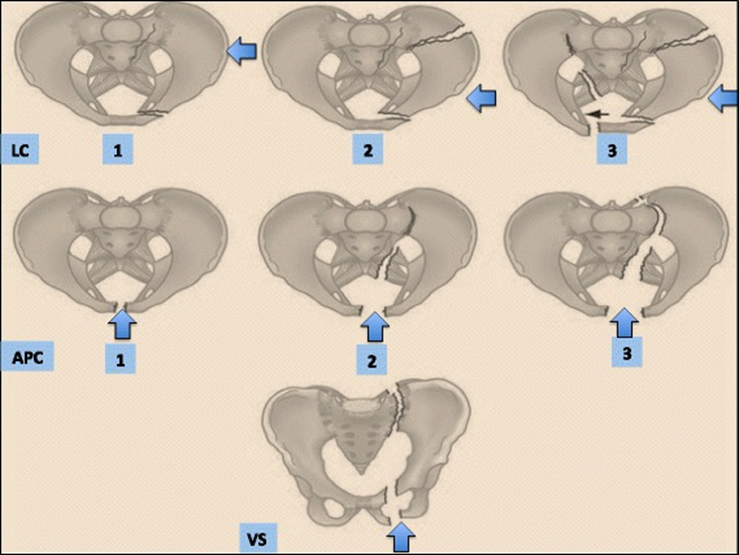
Classification for skeletal pelvic fractures. Image from (Coccolini,2017)
♦️LC – lateral compression
♦️APC- Antero-posterior compression:1 and 2
♦️VS -Vertical shear:2 down 2
▶️What is the treatment for a pelvic fracture in an elderly person
If treating pelvic fracture for the elderly it is important to strike a balance between two aspects.
1️⃣Proper bone consolidation and healing by not putting pressure on the fracture site.
2️⃣Not to lose physical function due to immobilisation and to avoid associated complications.
Treatment of pelvic fractures is usually based on some of these factors:
♦️The kind of pattern of the fracture.
♦️How many bones are displaced
♦️Your overall health.
♦️Other associated injuries.
There are two types of treatment used to manage pelvic fractures. If your fracture is stable, conservative management will be recommended and if it’s unstable the surgery may be an option.
Surgery for elderly patients is rare, treatment is often conservative and focuses on gradually resuming mobility as quickly as possible.
Conservative management:
When your have fractured your pelvis ring bones it will be difficult for you to bear weight on your legs:
🟣In the first days you may be advised to bed rest for 10 to 12 weeks if your fractures were caused by a major accident. and restricted sitting for to long if you are younger
However, this is less common in older patients due to the higher risk of deconditioning
Your orthopaedic doctor or surgeon will provide you with guidelines on the course of action.
Do you need:
🟣Guided mobilization with partial weight bearing if possible: using walking aids:
You will have to use crutches to help you move around for the next 3 months or until your bones have well consolidated.
🟣Wheelchair: in some cases you may need a wheelchair to help you move around and help you not put weight on the legs.
🟣Osteoanabolic medication to help with pain and reduce the risk of blood clots that may form in the veins of your legs and pelvis.
Kuper, 2019

X-ray image showing a dislocated fracture of the anterior pelvic ring Kuper,2019
Surgical options:
If your fractures are unstable, your doctor may suggest an operation to stabilise the fractures.
🟣External fixation using nails, screws plates and metal pins will be used to stabilise your fracture

X-ray image showing plates and screws used to repair the pelvis fractures: Image from Mullis,2012
▶️What are the possible complications after a pelvic fracture in the elderly
🟡Bleeding from pelvic fractures can occur from veins (80%) and from arteries (20%) and from bone fractures (Coccolini,2017)
🟡Wound healing problems
🟡Infection
🟡Damage to the nerve
🟡Pulmonary embolism, a blood clot in the lungs.
Kuper,2019
The aim of all treatment options whether non-operative or surgical must be the mobilization of your fracture, as quickly as possible so that you can get back to your normal activities.
What should be avoided during pelvic fractures
🟣After a hip or pelvic fracture, your doctor may advise you not to put any weight on the affected hip for six weeks or more.
🟣No weight bearing or toe touch weight bearing are usually chosen in the initial management to allow fracture and ligament healing and avoid fracture displacement and fixation failure
🟣So, a sponge bath or a shower chair is often necessary instead of a full shower or bath to avoid fracture displacement in the initial stages.
So as your healing progresses you should be patient and be hope full because before you know it, you will be back to you
▶️What is the fastest way to heal a broken pelvis
The truth is there is no single fastest way to heal a broken pelvis.
Recovery will depend on the severity of the injury, your age, overall health and the type of treatment received.
Healing will be assessed basing on clinical examination, x-rays and CT scans by your doctor
However there are some things you can do to help with the healing process.
🟣Follow your doctors’ instructions if you are told to rest as the healing takes off, please do so this will help with healing.
🟣Eat a well-balanced diet
🟣Reduce smoking during the time of recovery.
▶️What is the rehabilitation process for a pelvic fracture?
Usually in elderly patients’ rehabilitation process consists of three major pillars whether you had non conservative or surgery treatment.
1️⃣Mobilisation is normally started as early as possible with the help of physiotherapy. The aim is to help you get back to your feet and ask any questions you may have.
2️⃣Analgesia: this aim of this is to get you out of bed as soon as possible
3️⃣Osteoporotic medication such as vitamin D and calcium supplements to help with quick healing.
Initially you may not be able to start physiotherapy sessions, but you may need an assessment to see what you can do.
Your physiotherapy may be sent home for a follow up after you are discharged in hospital in the following weeks.
▶️What does physiotherapy rehabilitation involve?
A physiotherapy job is to assess when you can begin rehabilitation.
🟠If it is ok for you to start walking or perform simple exercises
🟠To show you simple tips on how to get out of bed
🟠How to move safely without excessive pain
🟠How to use the bathroom and maintain personal hygiene.
🟠If you are elderly, you may have had difficult balancing and walking before the fall.so it is important to be assessed before you resume walking again.
▶️When should rehabilitation begin?
Rehabilitation will depend on the type of fracture you have and your ability post injury.
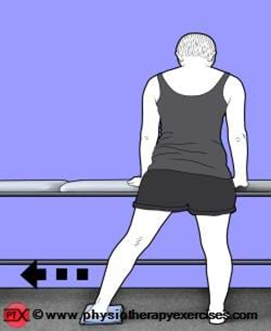
Simple exercises for pubic fracture from www.physiotherapy.com
To strengthen your hip muscles.
1️⃣Position yourself lying on your back with your knees bent. Tighten the muscles in your bottom and lift your bottom off the bed.

2️⃣Position yourself standing with your feet together. Start with your leg beside your body. Lift your leg out to the side. Ensure that you keep your body upright and your toes pointing forward

3️⃣Position yourself standing with your hands resting on a table in front of you. Take your leg back with your knee straight and body upright.

4️⃣Position yourself sitting on a chair with your arms crossed and feet shoulder width apart. Bring your shoulders forwards and stand up. Stick your bottom back and return to sitting.

Precautions: Place the chair against a wall.
5️⃣Position yourself standing, holding onto the back of a chair or table. Start with your feet together. Slide your unaffected leg sideways while slightly bending your affected knee and then slide your affected leg in.
▶️Is it normal to experience pain after a pelvic fracture?
It is very normal to experience pain after a pelvic fracture, this pain is often aggravated by moving the hip or attempting to walk.
This pain may also be caused by swelling or bruising in the hip area. But this does not mean that it will take long for you to recover.
The pain will decrease over the course of days, weeks or rarely months.
Here are a few things that will help ease the pain.
🟤Applying cold packs to the painful areas
🟤Proper positioning in bed and in the chair. Don’t hesitate to use a lot of pillows for support.
🟤Regular movement.
🟤Using a walker, crutches, or a walking frame to relieve pressure. Also, using armrests and handles for sitting and getting up.
🟤Taking pain medication prescribed by your doctor.
The pain is very common after a fractured pelvis, and it is not usually a sign of complication or concern. It will decrease over time as the days go by.
▶️When can one start walking again after a pelvic fracture
Your doctor will inform you if you are allowed to walk immediately or not.
I have seen patients who have been instructed to walk. In the first few weeks they are not allowed to put pressure on the leg, so they use crutches or wheelchairs to move around.
Those who have been instructed not to walk, the duration could take one month or 2 to 3 months until you are free of pain and complete healing.
Therefore, early weight bearing might be of advantage in many pelvic and acetabular fractures treatment.
Many studies report that in case of stable and partially unstable pelvic ring fractures early weight bearing can be allowed without progression of fracture displacement
Usually 24 hours after surgery, you are normally encouraged to stand and walk with minimum weight on the ground with the help of a rehabilitation therapist.
If at that moment you cannot tolerate the pain, the time to weight-bearing is postponed ensuring you are safe.
The major concern about early weight bearing is the risk of fixation failure and fracture displacement.

Postoperative pelvis X-rays(B) in standard view C) Clinical pictures of the patient walking with partial weight bearing on the left side and full weight bearing on the right side 7 days after surgery. (Murena, 2021)
▶️ Recovery time-line of pelvic fractures in the elderly.
| phase | Recovery time |
| Reduction in pain | A few days to weeks |
| Weight bearing restriction after surgery of acetabular fractures.Weight bearing for conservative treatment | 10-12 weeks after surgery (Murena,2021)Allowed weight bearing within 4 weeks after treatment. |
| Walking with crutches | immediate partial weight bearing for 8-12 weeks, starting from 2nd postoperative day. (Murena,2021) |
| Walking without crutches | 6 to 12 weeks will depend on how you feel. |
| Length of hospital stay | Type III or severe fracture was significantly longer than minor types (Omichi 2022) A study done in the United Kingdom indicated 18 days while other studies give a shorter average duration of 10 to 13 days depending on the severity of the fracture (Source: Wu 2020). |
| Bone healing | 6 to 12 weeks |
| Full functional & muscular recovery | Within 2 months to 1 year. |
Proposed recovery timeline of pelvis fracture.
▶️What is the life expectancy after a pelvic fracture
To date there are hundreds of studies dedicated to this topic and numerous publications that summarise these studies
I have selected study syntheses that in my opinion provided better answers to this question.
Date on life expectancy in other countries.
🟧 United Kingdom: A review undertaken 2018, The mean age of patients sustaining hip fractures continues to be steadily increasing at approximately just over 1 year of age for every 5-year period.
🟧The mean age of patients sustaining hip fractures increased from 73 years (1960s) to 81 years (2000s) to 82 years (2010s).
🟧 Over the six-decade period one-year mortality has reduced from an overall mean of 27% (1960s) to 20% (2010s).
20% of one year mortality means that out of 100 people who have had a hip fracture,20 of them will pass away within 1 year following the fracture
🟩German: Retrospective analyses have shown that osteoporotic pelvic fractures are associated with decreased mobility and independence and with a one-year mortality ranging from 9.5% to 27%
🟦Austria: a nationwide retrospective study showed the mortality rate one year after the fracture was higher in men than in women (13.0% and 11.1%, respectively). Patients with pelvic fractures aged ≥65 years had a high risk of mortality compared to controls.
🟩United states: Data from the 2010s (Siada 2017): The mortality rate at 3 months for open pelvic fractures decreased between the 2000s and 2010s, from 44% to 16%.
🟦South korea: Data from the 1990s (Chong 1997): The overall mortality of patients with pelvic fractures was 10.5%, which is 1.4 times higher than that of other trauma patients during the same period without pelvic fractures. Mortality was significantly higher in patients over 60 years old (37% mortality vs. 8%).
🟧France: Based on data from a two-year period between 2015 and 2017, the mortality rate after a hip fracture in France is 20.2% (Papanicolas 2021).
| Country | One year mortality rate after pelvis fracture |
| United states | 26.7% |
| Canada | 22.9% |
| Australia | 21.5% |
| France | 20.2% |
One year mortality rate after hip fracture in other countries
The older you are and the more health issues you have before the fracture, the higher the risk of death from a pelvic fracture.
We have come to the end of this article with any questions in the comments section. Wishing your a quick recovery!🙋
📚Source:
Coccolini F, Stahel PF, Montori G, Biffl W, Horer TM, Catena F, Kluger Y, Moore EE, Peitzman AB, Ivatury R, Coimbra R, Fraga GP, Pereira B, Rizoli S, Kirkpatrick A, Leppaniemi A, Manfredi R, Magnone S, Chiara O, Solaini L, Ceresoli M, Allievi N, Arvieux C, Velmahos G, Balogh Z, Naidoo N, Weber D, Abu-Zidan F, Sartelli M, Ansaloni L. Pelvic trauma: WSES classification and guidelines. World J Emerg Surg. 2017 Jan 18;12:5. doi: 10.1186/s13017-017-0117-6. PMID: 28115984; PMCID: PMC5241998.
Baker JE, Werner NL, Burlew CC. Management of Pelvic Trauma. Surg Clin North Am. 2024 Apr;104(2):367-384. doi: 10.1016/j.suc.2023.10.001. Epub 2023 Nov 22. PMID: 38453308.
Mullis BH: Techniques of anterior pelvic fixation. Instructional Course Lecture 61. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2012, pp. 19-25.
Küper MA, Trulson A, Stuby FM, Stöckle U. Pelvic ring fractures in the elderly. EFORT Open Rev. 2019 Jun 3;4(6):313-320. doi: 10.1302/2058-5241.4.180062. PMID: 31312519; PMCID: PMC6598730.
Oberkircher L, Ruchholtz S, Rommens PM, Hofmann A, Bücking B, Krüger A. Osteoporotic Pelvic Fractures. Dtsch Arztebl Int. 2018 Feb 2;115(5):70-80. doi: 10.3238/arztebl.2018.0070. PMID: 29439771; PMCID: PMC5817189.
Omichi T, Takegami Y, Tokutake K, Saito Y, Ito O, Ando T, Imagama S. Mortality and functional outcomes of fragility fractures of the pelvis by fracture type with conservative treatment: a retrospective, multicenter TRON study. Eur J Trauma Emerg Surg. 2022 Aug;48(4):2897-2904. doi: 10.1007/s00068-021-01839-1. Epub 2021 Dec 1. PMID: 34850256.
Wu YT, Cheng CT, Tee YS, Fu CY, Liao CH, Hsieh CH. Pelvic injury prognosis is more closely related to vascular injury severity than anatomical fracture complexity: the WSES classification for pelvic trauma makes sense. World J Emerg Surg. 2020 Aug 17;15(1):48. doi: 10.1186/s13017-020-00328-x. PMID: 32807185; PMCID: PMC7433075.
Murena L, Canton G, Hoxhaj B, Sborgia A, Fattori R, Gulli S, Vaienti E. Early weight bearing in acetabular and pelvic fractures. Acta Biomed. 2021 Sep 2;92(4):e2021236. doi: 10.23750/abm.v92i4.10787. PMID: 34487095; PMCID: PMC8477081.
Behanova M, Haschka J, Reichardt B, Dimai HP, Resch H, Zwerina J, Kocijan R. Pelvic Fractures-An Underestimated Problem? Incidence and Mortality Risk after Pelvic Fracture in Austria, 2010-2018. J Clin Med. 2022 May 17;11(10):2834. doi: 10.3390/jcm11102834. PMID: 35628960; PMCID: PMC9146576.
Papanicolas I, Riley K, Abiona O, Arvin M, Atsma F, Bernal-Delgado E, Bowden N, Blankart CR, Deeny S, Estupiñán-Romero F, Gauld R, Haywood P, Janlov N, Knight H, Lorenzoni L, Marino A, Or Z, Penneau A, Schoenfeld AJ, Shatrov K, Stafford M, van de Galien O, van Gool K, Wodchis W, Jha AK, Figueroa JF. Differences in health outcomes for high-need high-cost patients across high-income countries. Health Serv Res. 2021 Dec;56 Suppl 3(Suppl 3):1347-1357. doi: 10.1111/1475-6773.13735. Epub 2021 Aug 11. PMID: 34378796; PMCID: PMC8579207.Haleem S, Choudri MJ, Kainth GS, Parker MJ. Mortality following hip fracture: Trends and geographical variations over the last SIXTY years. Injury. 2023 Feb;54(2):620-629. doi: 10.1016/j.injury.2022.12.008. Epub 2022 Dec 9. PMID: 36549980.