
I see so many patients who come for x-ray with thoracic lumbar pain querying back compression vertebral fracture. You might have just experienced one yourself.
Are you looking for answers about treatment, recovery and physiotherapy for thoracic lumbar compression fractures.
As a certified diagnostic radiographer, I will use my knowledge and rely on medical scientific studies to address the most frequently asked questions from my patients and internet users regarding the development of vertebral compression fractures.
At the end of the blog post, you will find references to the scientific publications and recommendations on which I rely.
Do you still have questions after reading this article? You can leave them in the comments, and I will be happy to respond!🙏
Happy reading!😀
Last updated: Sept 2024. Written by Juliet S, a diagnostic radiographer.
Before we delve deep into this article let’s first educate ourselves on:
▶️What are the different vertebrae on a spine?
We do have 33 bones that make up our spinal column, 24 of which are mobile and 9 of which are fused.
The mobile vertebrae make up the upper portion of the spinal column and include the 7 cervical, 12 thoracic, and 5 lumbar vertebrae make up the lower back.
The fused vertebrae make up the inferior portion of the spinal column and include the 5 sacral and 4 coccyx vertebrae.
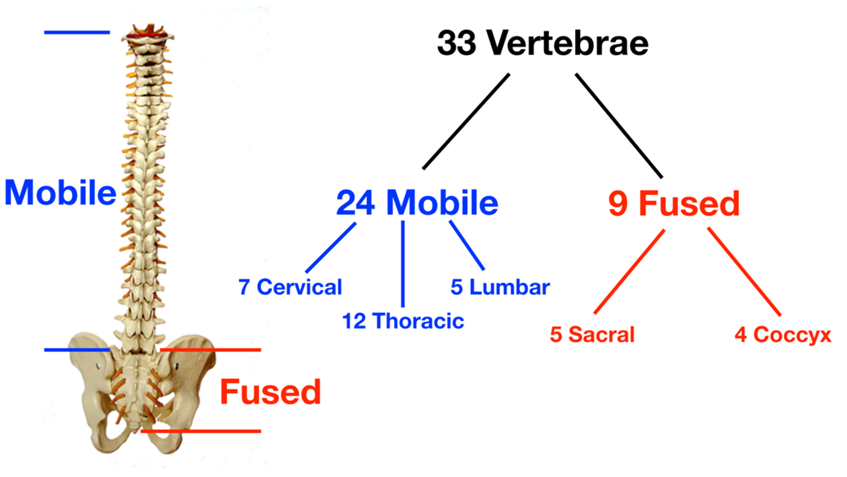
Image from: https://www.ezmedlearning.com
For this article we will be covering the 2 regions of the vertebral column that’s the thoracic and lumbar that are more prone to compression fractures.
These two regions, their treatment and evolution are generally the same.
It is possible to break one or more of these vertebrae at the sometime after a fall, an accident or sometimes without doing anything especially in the elderly people or if you have osteoporosis.
What does T 1, T2, T3, T 4 TO 12 and L1, L2, L3, L4, L5 mean
Depending on which vertebra is broken, the x-ray report will describe the vertebra as:
🟠Thorax spine vertebra T 5, T7, T11, T12 if you have broken the upper region.
🟠Lumbar spine vertebra L1, L2, L3, L4 and L5 if you have compressed the lower back.
All these vertebrae are bones, and they can fracture or compress, on different parts of vertebral bodies.
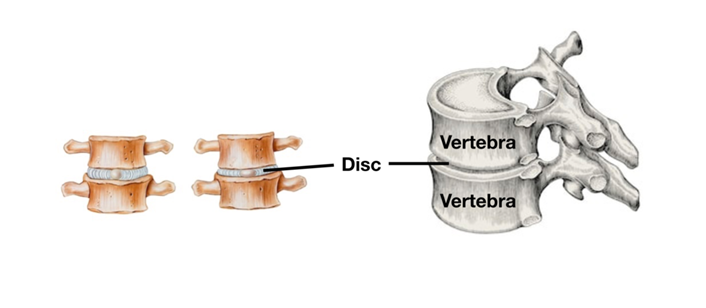
Image showing two vertebrae and disc that helps to support them.
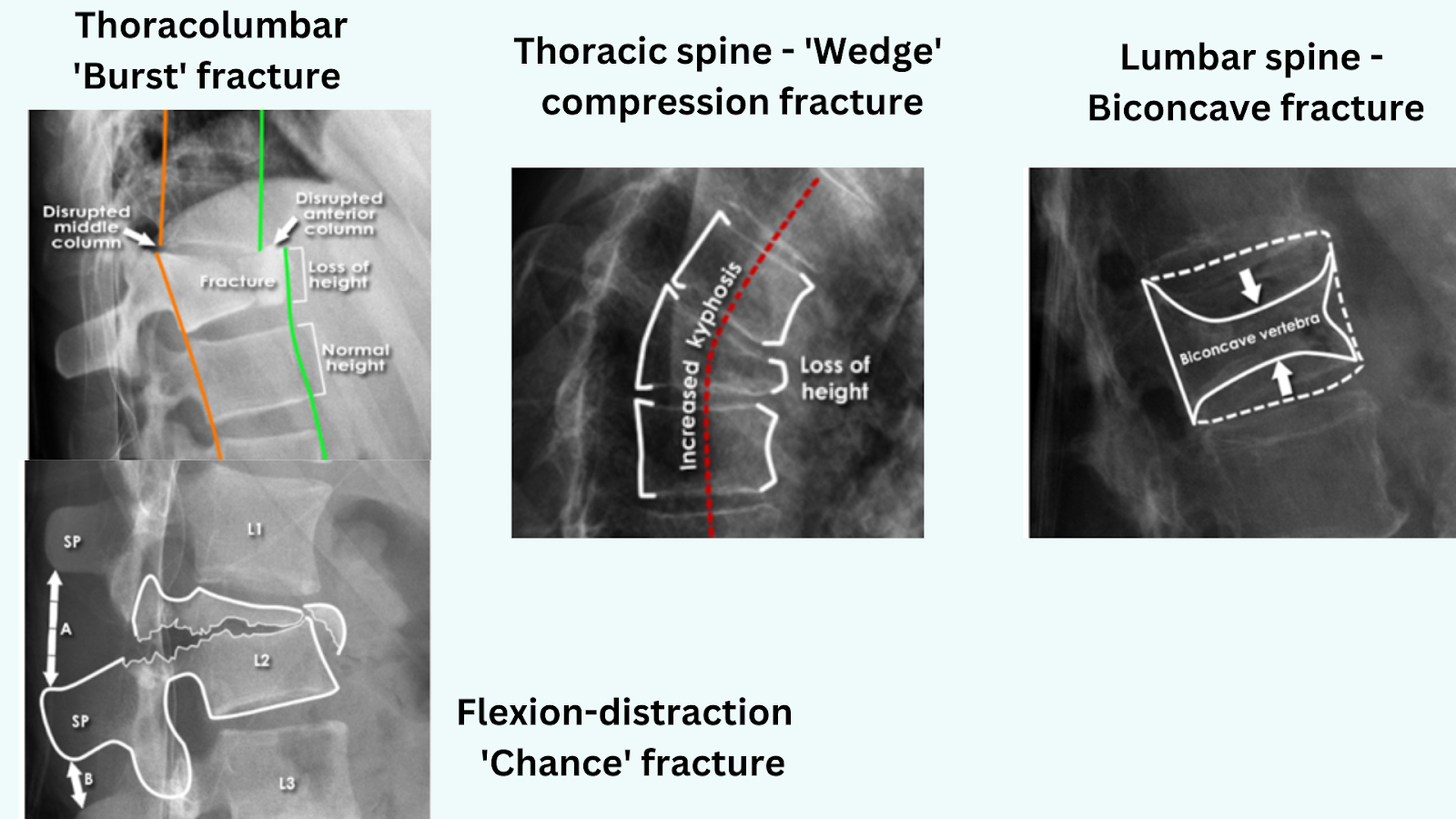
▶️What a the most common types of vertebral fractures:
♦️Compression fractures or osteoporosis
These fractures are small breaks or cracks in your vertebrae that are caused by traumas or develop over time because of osteoporosis.
♦️Burst fractures:
These fractures happen when your spine is suddenly compressed with a strong force. They can cause your vertebrae to break into many pieces.
♦️Chance or distraction fractures:
These are fractures that happen when your vertebrae are suddenly pulled away from each other. They’re almost like the opposite of a burst fracture.
Images of different types of vertebral fractures or compression.
▶️What causes vertebral compression fractures.
1️⃣Osteoporosis is a disease that thins the bones, often to the point that they are too weak to bear normal pressure. The thinning bones can collapse during normal activity, leading to a spinal compression fracture.
2️⃣Trauma to the spinal vertebrae can also lead to minor or severe fractures. Such trauma could come from a fall, a forceful jump, a car accident, or any event that stresses the spine past its breaking point.
3️⃣Tumours or metastatic disease is a term that refers to the spread of cancer cells into other areas of the body. The bones of the spine are a common place for many types of cancers to spread.
4️⃣Spinal infections can cause spinal fractures when it weakens the bone.
5️⃣Genetic disorders sometimes can lead to compressed fractures.
▶️ What are symptoms of vertebral compression fractures.
The main clinical symptoms of vertebral fractures typically include one or a combination of the following:
🟤Sudden onset of back pain.
🟤Worse pain while standing or walking.
🟤Less intense pain while lying on one’s back.
🟤Limited spinal mobility.
🟤Height loss.
🟤Deformity and disability.
▶️What are the potential consequences of a vertebral collapse?
Due to nonoperative management of these fractures, you may experience:
⚪Difficult to walk.
⚪You may find it difficult to do all the things you do daily.
⚪ It can lead to continued back pain and progression of a kyphotic deformity.
⚪There is a high likelihood of having a progression of vertebral body collapse in addition to having additional fractures in the future.
⚪If the spinal cord or nerves are affected during the fracture, you may experience bowel/bladder dysfunction along with numbness, tingling, or weakness in the arms or legs
The pain of acute fracture usually lasts 4 to 6 weeks with intense pain at the site of fracture.
Chronic pain may also occur in patients with multiple compression fractures, height loss and low bone density but is probably due to structural changes or osteoarthritis {Silverman 1992}
For those who are bothered, different treatments can be offered. Not based on what is seen on the x-ray, but rather on the discomfort: pain, loss of strength, etc.
The aims of acute management are to reduce symptoms and mobilise your fracture as quickly as possible to help maintain or increase skeletal mass and improve mobility and function.
▶️What complications can arise.
Here are the possible complications of a vertebral collapse according to studies and experience from patients.
✅Anatomical and chronic back pain.
Severe and chronic back pain most often originates in the lumbar intervertebral discs, the apophyseal joints, and the sacroiliac joints
This pain can occur suddenly or gradually over time and may be localised to the affected vertebrae or radiate throughout the back.
The pain may worsen when standing, walking, or twisting and may improve when lying down.
▶️What is the procedure to follow when treating vertebral compression fractures.
You will have a Magnetic resonance imaging (MRI) scan because it is the preferred modality for making the diagnosis and selecting the most appropriate treatment for vertebral fractures.
Usually the first options are:
➡️Conservative treatment.
You will be encouraged to bed rest and given strong medication to help settle the pain.
You will be given a back brace if the fracture is nondisplaced and minimally painful to prevent the compression fracture from progressing and to improve function during the fracture healing.
Using a bracing as management for osteoporotic vertebral fractures may have a small benefit for pain without increasing risk of harm (Bolton 2022)
➡️Conventional surgery
A surgeon may recommend open surgery to relieve pressure on the nerves or the spinal cord, both of which pass through the spinal canal formed by the stacked vertebrae.
This procedure is called decompression where a direct access to the spine through an incision will be done to stabilise the spinal bones surrounding the fracture.
Or a surgeon may perform spinal fusion to permanently join two or more vertebrae together to eliminate movement between them.
➡️Minimally invasive techniques such as:
♦️Percutaneous Vertebroplasty/ cementoplasty and kyphoplasty there treatment is more of the same.
These are minimally recommended invasive procedures used to restore height and reduce fractures in vertebral body compression fractures. They may help with the pain and discomfort
Vertebroplasty is very similar to kyphoplasty, except a balloon is not used to create an empty cavity within the vertebral space.
The surgeon inserts the cannula into the vertebra, using a live X-ray image to guide its placement, and injects the soft cement-like material directly into the vertebral fracture.
This cement also hardens quickly, eliminating painful movement of the fractured bone.
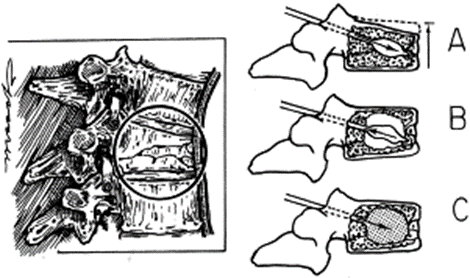
Kyphoplasty
These kinds of procedures are done under Anastasias where the collapsed vertebral body is accessed through a transpedicular route (A). The balloon at the end of the instrument is inflated, thus restoring the height of the body. (B).
In (C)The balloon is removed, and the defect is filled with bone cement (polymethylmethacrylate), which re-establishes structural integrity to the vertebral body.
▶️What to expect after surgery
Recovery from kyphoplasty or vertebroplasty is minimal. Most people can walk on their own and return home hours after surgery. Most people are fully recovered and free of back pain in five days or more.
Postoperative pain is typically managed using pain relief medication prescribed by your doctor.
You will be given a follow-up appointment two weeks after surgery, where your spine will be examined, sometimes using X-rays to inspect the cement.
By this time, most people feel well enough to return to everyday activities, including a regular exercise routine.
▶️How effective are these operations
There are a few studies that compare the evaluation of people with compression fractures operated or not operated on.
The idea is to see if people who have had surgery feel better afterwards than others. Otherwise, what’s the point of doing this surgical procedure (with the possible complications), even if it makes sense in theory?
Here are some of the conclusions from recent studies.
Both conservative and surgical treatments showed successful clinical results at the end of the 1-year follow-up period. Kyphoplasty showed better outcomes in the first month only.
Kyphoplasty is becoming a common treatment for painful osteoporotic compression fractures and some people have shown numerous benefits, such as early pain control and height restoration of the collapsed vertebral body.
A total of 259 patients were enrolled, and 231 patients (82 of 91 patients in the kyphoplasty group and 149 of 168 patients in the conservative treatment group completed the 1-year follow-up
Some people claim to have better outcomes in the first month only after the procedure. However, there were no significant differences in outcome measures between the two groups at 3, 6, or 12 months
And some studies base on these results, not to recommend kyphoplasty if a conservative treatment can be used.
The American Society of Bone and Mineral Research recommends not using kyphoplasty or vertebroplasty in acute osteoporotic compression fractures.
Because the bones are too thin and fragile to be subjected to such treatments.
Another contraindication of kyphoplasty is not to use it if you have severe vertebral fracture or when the facet joint has been involved in the fracture
No benefit for health-related quality of life and activity measures were demonstrated for conservative interventions or surgical multimodal interventions.
Based on my professional knowledge, I tend to believe that this surgical procedure does not offer significant benefits, apart from providing something new to try for individuals who are suffering.
♦️Physiotherapy and rehabilitation of a vertebral compression fracture.
The best way to benefit from conservative therapy and prevent compression fractures in the first three months is to have an active lifestyle, proper nutrition which includes oral calcium and vitamin D for at least 4 years.
(Zileli 2022).
You can try doing little exercises as your back pain allows, this can help you relieve pain more than doing nothing at all. There is no one or even some specific exercises recommended better than others.
What matters is to find the physical activity that helps you move your muscles, joints and heart enough in relation to your level without causing you more pain.
♦️Natural treatment
The best natural treatment remains the passage of time and maintaining minimal physical activity.
But a healthy diet full of proteins and calcium can help strengthen bones.so changing your diet to a healthy one may help to strengthen bones.
▶️How long does it take for a collapsed vertebral back to heal?
Spinal vertebral fractures are different from broken arms or legs, their healing time can take more than 6 weeks this is because they are more complex bones.
Recovery can take much longer if surgery was done. You will lose some height and have a more bent back.
Reasons why consolidation may take longer.
🟧 When you fracture a vertebral bone, you may also cause damage to the spinal cord or nerves because of the compression
🟧The muscles and tendons surrounding can be strained and damaged.
🟧Remember your spine supports your body weight and more often in motion of bending and twisting.
🟧Also bone density decreases with age, healing in this case may take longer.
Healing will depend on how severe your vertebral damage is and what kind of treatment you are given.
For many people, a spinal compression fracture will hurt less as the bone heals. That can take up to 2 or 3 months or more.
Other people will still have pain after the fracture has healed. Some people feel almost no symptoms from spinal compression fracture
The consolidation process may take several months, but it doesn’t necessarily prohibit activity during the recovery period.
Fractures due to osteoporosis often become less painful with rest and pain medicines
It’s important to note that these data may be more personalised than the actual reality. This is because clinical studies often include and follow individuals with more severe conditions.
Some people with vertebral compression may not even seek medical attention.
To help with your healing you can avoid doing any repetitive bending or twisting or lifting anything more than 20 pounds for three months.
▶️Can you walk with a vertebral compression fracture?
Depending on what caused your vertebral compression fracture and which type of fracture you have.
You’ll still be able to walk with a broken compression back If the cause was not sudden trauma. It might be painful or make your pain worse.
In some cases, older adults with vertebral compression fractures have difficulty walking because of declines in their physical and mental functions caused by treatment and bed rest.
Which may require long-term rehabilitation for them to walk again.
▶️Can you fracture your back and not know it?
Spine fractures can be painful, but those that develop gradually may cause no symptoms at first.
Some people realise they have a compression fracture only when it’s detected by an X-ray performed for another reason.
If the fracture progresses, a person may experience dull back pain that gets worse during movement.
We have come to the end of this article, wishing you a quick recovery!🙋
📚Sources:
Silverman SL. The clinical consequences of vertebral compression fracture. Bone. 1992;13 Suppl 2:S27-31. doi: 10.1016/8756-3282(92)90193-z. PMID: 1627411.
Kurita M, Fujita T, Kasahara R, Yamamoto Y, Ohira Y, Otsuki K, Morishita S. Prediction of Walking Independence in Older Women with Vertebral Compression Fracture Using Phase Angle: A Preliminary Study Using Propensity Score. Prog Rehabil Med. 2024 Jan 30;9:20240004. doi: 10.2490/prm.20240004. PMID: 38292562; PMCID: PMC10823123.
Adams MA. Biomechanics of back pain. Acupunct Med. 2004 Dec;22(4):178-88. doi: 10.1136/aim.22.4.178. PMID: 15628775.
Prost S, Pesenti S, Fuentes S, Tropiano P, Blondel B. Treatment of osteoporotic vertebral fractures. Orthop Traumatol Surg Res. 2021 Feb;107(1S):102779. doi: 10.1016/j.otsr.2020.102779. Epub 2020 Dec 13. PMID: 33321233.
Zileli M, Fornari M, Costa F, Anania CD, Parthiban J, Sharif S. Epidemiology, natural course, and preventive measures of osteoporotic vertebral fracture. wfns Spine Committee Recommendation . J Neurosurg Sci. 2022 Aug;66(4):282-290. doi:10.23736/S0390-5616.22.05643-0. Epub 2022 AUG 17. PMID: 35301844.
Alsoof D, Anderson G, McDonald CL, Basques B, Kuris E, Daniels AH. Diagnosis and Management of Vertebral Compression Fracture. Am J Med. 2022 Jul;135(7):815-821. doi: 10.1016/j.amjmed.2022.02.035. Epub 2022 Mar 18. PMID: 35307360.
Boss S, Srivastava V, Anitescu M. Vertebroplasty and Kyphoplasty. Phys Med Rehabil Clin N Am. 2022 May;33(2):425-453. doi: 10.1016/j.pmr.2022.01.008. PMID: 35526978.
Bolton K, Wallis JA, Taylor NF. Benefits and harms of non-surgical and non-pharmacological management of osteoporotic vertebral fractures: A systematic review and meta-analysis. Braz J Phys Ther. 2022 Jan-Feb;26(1):100383. doi: 10.1016/j.bjpt.2021.100383. Epub 2022 Jan 10. PMID: 35063701; PMCID: PMC8784306.
Images from; https://www.radiologymasterclass.co.uk